Randi J Ryan, Andrew J Bentall, Naim Issa, Patrick G Dean, Byron H Smith, Mark D Stegall, Samy M Riad
{"title":"Outcomes of Older Primary Kidney Transplant Recipients by Induction Agent and High-risk Viral Discordance Status in the United States.","authors":"Randi J Ryan, Andrew J Bentall, Naim Issa, Patrick G Dean, Byron H Smith, Mark D Stegall, Samy M Riad","doi":"10.1097/TXD.0000000000001698","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The impact of induction type or high-risk viral discordance on older kidney transplant recipients is unclear. Herein, we analyzed the association between induction type, viral discordance, and outcomes for older recipients.</p><p><strong>Methods: </strong>We analyzed the Scientific Registry of Transplant Recipients standard analysis file for all primary kidney transplant recipients older than 55 y who were transplanted between 2005 and 2022. All transplants were crossmatch negative and ABO-compatible. Recipients were discharged on tacrolimus and mycophenolate ± steroids. Recipients were categorized into 3 groups by induction received: rabbit antithymocyte globulin (r-ATG; N = 51 079), interleukin-2 receptor antagonist (IL-2RA; N = 22 752), and alemtuzumab (N = 13 465). Kaplan-Meier curves were generated for recipient and graft survival, and follow-up was censored at 10 y. Mixed-effect Cox proportional hazard models examined the association between induction type, high-risk viral discordance, and outcomes of interest. Models were adjusted for pertinent recipient and donor characteristics.</p><p><strong>Results: </strong>Induction type did not predict recipient survival in the multivariable model, whereas Epstein-Barr virus high-risk discordance predicted 14% higher mortality (1.14 [1.07-1.21], <i>P</i> < 0.01). In the multivariable model for death-censored graft survival, alemtuzumab, but not IL-2RA, was associated with an increased risk of graft loss (1.18 [1.06-1.29], <i>P</i> < 0.01) compared with r-ATG. High-risk cytomegalovirus discordance predicted 10% lower death-censored graft survival (1.10 [1.01-1.19], <i>P</i> < 0.02). Live donor and preemptive transplantation were favorable predictors of survival.</p><p><strong>Conclusions: </strong>In this large cohort of older transplant recipients, alemtuzumab, but not IL-2RA, induction was associated with an increased risk of graft loss compared with r-ATG. Cytomegalovirus and Epstein-Barr virus high-risk viral discordance portended poor graft and recipient survival, respectively.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"10 10","pages":"e1698"},"PeriodicalIF":1.9000,"publicationDate":"2024-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11427033/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001698","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
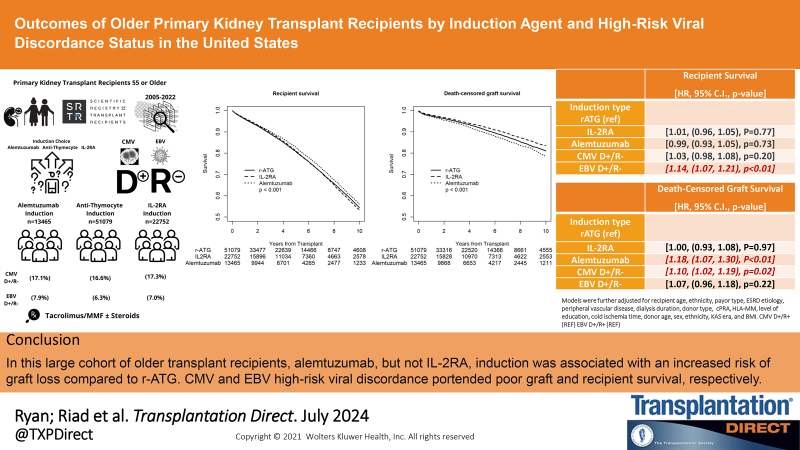
Background: The impact of induction type or high-risk viral discordance on older kidney transplant recipients is unclear. Herein, we analyzed the association between induction type, viral discordance, and outcomes for older recipients.
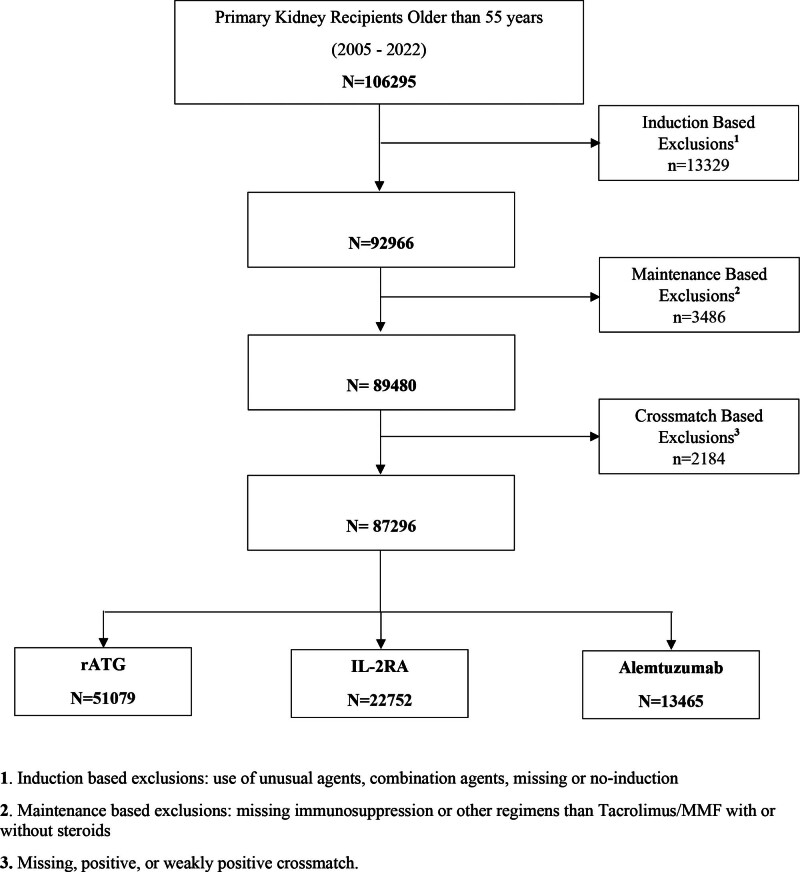
Methods: We analyzed the Scientific Registry of Transplant Recipients standard analysis file for all primary kidney transplant recipients older than 55 y who were transplanted between 2005 and 2022. All transplants were crossmatch negative and ABO-compatible. Recipients were discharged on tacrolimus and mycophenolate ± steroids. Recipients were categorized into 3 groups by induction received: rabbit antithymocyte globulin (r-ATG; N = 51 079), interleukin-2 receptor antagonist (IL-2RA; N = 22 752), and alemtuzumab (N = 13 465). Kaplan-Meier curves were generated for recipient and graft survival, and follow-up was censored at 10 y. Mixed-effect Cox proportional hazard models examined the association between induction type, high-risk viral discordance, and outcomes of interest. Models were adjusted for pertinent recipient and donor characteristics.
Results: Induction type did not predict recipient survival in the multivariable model, whereas Epstein-Barr virus high-risk discordance predicted 14% higher mortality (1.14 [1.07-1.21], P < 0.01). In the multivariable model for death-censored graft survival, alemtuzumab, but not IL-2RA, was associated with an increased risk of graft loss (1.18 [1.06-1.29], P < 0.01) compared with r-ATG. High-risk cytomegalovirus discordance predicted 10% lower death-censored graft survival (1.10 [1.01-1.19], P < 0.02). Live donor and preemptive transplantation were favorable predictors of survival.
Conclusions: In this large cohort of older transplant recipients, alemtuzumab, but not IL-2RA, induction was associated with an increased risk of graft loss compared with r-ATG. Cytomegalovirus and Epstein-Barr virus high-risk viral discordance portended poor graft and recipient survival, respectively.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


