Antal van der Gaag, Steven P Cohen, Milan P Stojanovic, Frank J P M Huygen, Jan Willem Kallewaard
{"title":"12. Vascular pain: Ischemic pain in the extremities and Raynaud's syndrome","authors":"Antal van der Gaag, Steven P Cohen, Milan P Stojanovic, Frank J P M Huygen, Jan Willem Kallewaard","doi":"10.1111/papr.13421","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Peripheral artery diseases (PAD) and Raynaud's syndrome are associated with substantial morbidity. PAD, through the restriction of blood flow to the extremities, may lead to critical limb ischemia with symptoms of pain at rest which may eventually progress to severe limb ischemia with gangrene. This serious and painful clinical condition requires extensive medical care, is limb-threatening and, in case of delayed or unsuccessful treatment, is associated with a high mortality rate. In Raynaud's syndrome, the blood supply to certain parts of the body, usually the fingers and toes and less frequently the nose or ears, is restricted because of vasculopathy of the smaller vessels at acral sites. Under certain circumstances, with cold as the most well-known provoking factor, blood flow restriction occurs, leading to demarcated color changes and symptoms such as pain, paresthesia, and numbness. In severe cases of Raynaud syndrome tissue ischemia may lead to necrosis and the need for amputation of the affected area.</p><p><strong>Methods: </strong>In this narrative review, the literature on the diagnosis and interventional pain treatment of PAD and Raynaud's syndrome was updated and summarized.</p><p><strong>Objectives: </strong>This review focused on interventional pain treatment. In PAD, the effects of the intervention on limb salvage, ulcer healing, and ischemic pain were summarized. Additionally, results with respect to skin microcirculation and quality of life were reported if available. In Raynaud's syndrome, we focused on the effect of the intervention on peripheral blood flow metrics and pain intensity during attacks.</p><p><strong>Results: </strong>In PAD, prevention and treatment of risk factors are important. Initially, conservative treatment and pharmacological therapy are preferred first-line therapies. However, when disease progression occurs, interventional management may be considered. The literature search yielded conflicting evidence for sympathectomy as a treatment for PAD. Spinal cord stimulation (SCS) as a treatment modality for advanced PAD had high-quality evidence for limb salvage in subgroups of patients but conflicting evidence for other outcome measures such as pain, wound healing, and quality of life. The literature search for interventional pain management in Raynaud's syndrome was limited to only one randomized controlled trial (RCT) studying the effect of thoracic sympathectomy. This study had several limitations and hence the level of evidence for this interventional treatment is very low. No RCTs studying SCS in patients with Raynaud's syndrome were found.</p><p><strong>Conclusions: </strong>In both PAD and Raynaud's syndrome, additional RCTs are needed to substantiate interventional (pain) management and bolster the evidence base for sympathectomy and SCS as treatment options.</p>","PeriodicalId":19974,"journal":{"name":"Pain Practice","volume":" ","pages":""},"PeriodicalIF":2.7000,"publicationDate":"2024-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11683193/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pain Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/papr.13421","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Peripheral artery diseases (PAD) and Raynaud's syndrome are associated with substantial morbidity. PAD, through the restriction of blood flow to the extremities, may lead to critical limb ischemia with symptoms of pain at rest which may eventually progress to severe limb ischemia with gangrene. This serious and painful clinical condition requires extensive medical care, is limb-threatening and, in case of delayed or unsuccessful treatment, is associated with a high mortality rate. In Raynaud's syndrome, the blood supply to certain parts of the body, usually the fingers and toes and less frequently the nose or ears, is restricted because of vasculopathy of the smaller vessels at acral sites. Under certain circumstances, with cold as the most well-known provoking factor, blood flow restriction occurs, leading to demarcated color changes and symptoms such as pain, paresthesia, and numbness. In severe cases of Raynaud syndrome tissue ischemia may lead to necrosis and the need for amputation of the affected area.
Methods: In this narrative review, the literature on the diagnosis and interventional pain treatment of PAD and Raynaud's syndrome was updated and summarized.
Objectives: This review focused on interventional pain treatment. In PAD, the effects of the intervention on limb salvage, ulcer healing, and ischemic pain were summarized. Additionally, results with respect to skin microcirculation and quality of life were reported if available. In Raynaud's syndrome, we focused on the effect of the intervention on peripheral blood flow metrics and pain intensity during attacks.
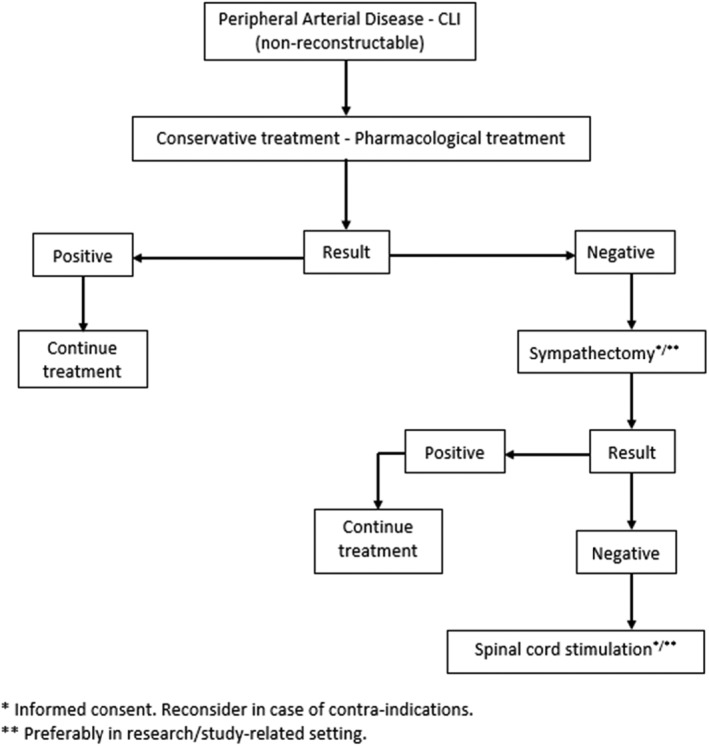
Results: In PAD, prevention and treatment of risk factors are important. Initially, conservative treatment and pharmacological therapy are preferred first-line therapies. However, when disease progression occurs, interventional management may be considered. The literature search yielded conflicting evidence for sympathectomy as a treatment for PAD. Spinal cord stimulation (SCS) as a treatment modality for advanced PAD had high-quality evidence for limb salvage in subgroups of patients but conflicting evidence for other outcome measures such as pain, wound healing, and quality of life. The literature search for interventional pain management in Raynaud's syndrome was limited to only one randomized controlled trial (RCT) studying the effect of thoracic sympathectomy. This study had several limitations and hence the level of evidence for this interventional treatment is very low. No RCTs studying SCS in patients with Raynaud's syndrome were found.
Conclusions: In both PAD and Raynaud's syndrome, additional RCTs are needed to substantiate interventional (pain) management and bolster the evidence base for sympathectomy and SCS as treatment options.
导言:外周动脉疾病(PAD)和雷诺综合征与严重的发病率有关。PAD 通过限制肢体血流,可能导致肢体严重缺血,并伴有静息时疼痛的症状,最终可能发展为肢体严重缺血并伴有坏疽。这种严重而痛苦的临床症状需要广泛的医疗护理,会危及肢体,如果治疗延误或不成功,死亡率很高。在雷诺氏综合征中,身体某些部位(通常是手指和脚趾,较少见的是鼻子或耳朵)的血液供应受到限制,原因是尖锐部位的小血管发生病变。在某些情况下,最常见的诱发因素是寒冷,血流受限会导致明显的颜色变化以及疼痛、麻痹和麻木等症状。在雷诺综合征的严重病例中,组织缺血可能导致坏死,需要截肢:在这篇叙事性综述中,对有关 PAD 和雷诺综合征的诊断和介入性疼痛治疗的文献进行了更新和总结:本综述侧重于介入性疼痛治疗。在 PAD 中,总结了干预对肢体挽救、溃疡愈合和缺血性疼痛的影响。此外,还报告了皮肤微循环和生活质量方面的结果(如果有的话)。对于雷诺氏综合征,我们重点研究了干预措施对外周血流指标和发作时疼痛强度的影响:结果:对于 PAD,预防和治疗危险因素非常重要。最初,保守治疗和药物治疗是首选的一线疗法。然而,当疾病进展时,可考虑进行介入治疗。文献检索结果显示,交感神经切除术作为 PAD 治疗方法的证据相互矛盾。脊髓刺激(SCS)作为晚期 PAD 的一种治疗方式,在亚组患者的肢体挽救方面有高质量的证据,但在疼痛、伤口愈合和生活质量等其他结局指标方面的证据相互矛盾。有关雷诺氏综合征介入性疼痛治疗的文献搜索仅限于一项研究胸交感神经切除术效果的随机对照试验(RCT)。该研究存在一些局限性,因此这种介入治疗的证据水平很低。没有发现研究雷诺氏综合征患者SCS的随机对照试验:结论:对于 PAD 和雷诺氏综合征,需要更多的 RCT 来证实介入性(疼痛)治疗,并加强交感神经切除术和 SCS 作为治疗方案的证据基础。
期刊介绍:
Pain Practice, the official journal of the World Institute of Pain, publishes international multidisciplinary articles on pain and analgesia that provide its readership with up-to-date research, evaluation methods, and techniques for pain management. Special sections including the Consultant’s Corner, Images in Pain Practice, Case Studies from Mayo, Tutorials, and the Evidence-Based Medicine combine to give pain researchers, pain clinicians and pain fellows in training a systematic approach to continuing education in pain medicine. Prior to publication, all articles and reviews undergo peer review by at least two experts in the field.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


