Adherence to clinical care standards and mortality after hip fracture surgery in New South Wales, 2015–2018: a retrospective population-based study
Abstract
Objectives
To determine whether adherence to hip fracture clinical care quality indicators influences mortality among people who undergo surgery after hip fracture in New South Wales, both overall and by individual indicator.
Study design
Retrospective population-based study; analysis of linked Australian and New Zealand Hip Fracture Registry (ANZHFR), hospital admissions, residential aged care, and deaths data.
Setting, participants
People aged 50 years or older with hip fractures who underwent surgery in 21 New South Wales hospitals participating in the ANZHFR, 1 January 2015 – 31 December 2018.
Main outcome measures
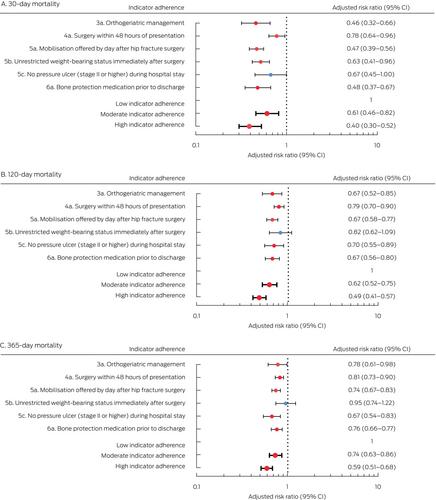
Thirty-day (primary outcome), 120-day, and 365-day mortality (secondary outcomes) by clinical care indicator adherence level (low: none to three of six indicators achieved; moderate: four indicators achieved; high: five or six indicators achieved) and by individual indicator.
Results
Registry data were available for 9236 hip fractures in 9058 people aged 50 years or older during 2015–2018; the mean age of patients was 82.8 years (standard deviation, 9.3 years), 5510 patients were women (69.4%). Complete data regarding adherence to clinical care indicators were available for 7951 fractures (86.1%); adherence to these indicators was high for 5135 (64.6%), moderate for 2249 (28.3%), and low for 567 fractures (7.1%). After adjustment for age, sex, comorbidity, admission year, pre-admission walking ability, and residential status, 30-day mortality risk was lower for high (adjusted relative risk [aRR], 0.40; 95% confidence interval [CI], 0.30–0.52) and moderate indicator adherence hip fractures (aRR, 0.61; 95% CI, 0.46–0.82) than for low indicator adherence hip fractures, as was 365-day mortality (high adherence: aRR, 0.59 [95% CI, 0.51–0.68]; moderate adherence: aRR, 0.74 [95% CI, 0.63–0.86]). Orthogeriatric care (365 days: aRR, 0.78; 95% CI, 0.61–0.98) and offering mobilisation by the day after surgery (365 days: aRR, 0.74; 95% CI, 0.67–0.83) were associated with lower mortality risk at each time point.
Conclusions
Clinical care for two-thirds of hip fractures attained a high level of adherence to the six quality care indicators, and short and longer term mortality was lower among people who received such care than among those who received low adherence care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


