André Alexandre, David Sá-Couto, Mariana Brandão, Sofia Cabral, Tomás Fonseca, Rita Quelhas Costa, António Marinho, Carlos Vasconcelos, Betânia Ferreira, João Pedro Ferreira, Patrícia Rodrigues
{"title":"Subclinical left ventricular dysfunction in rheumatoid arthritis: findings from the prospective Porto-RA cohort.","authors":"André Alexandre, David Sá-Couto, Mariana Brandão, Sofia Cabral, Tomás Fonseca, Rita Quelhas Costa, António Marinho, Carlos Vasconcelos, Betânia Ferreira, João Pedro Ferreira, Patrícia Rodrigues","doi":"10.1007/s00392-024-02548-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>Patients with rheumatoid arthritis (RA) have an increased risk of cardiac dysfunction and heart failure (HF) due to a pro-inflammatory state. Detecting cardiac dysfunction in RA is challenging as these patients often present preserved ejection fraction (EF) but may have subclinical ventricular dysfunction. Echocardiographic strain analysis is a promising tool for early detection of subclinical left ventricular systolic dysfunction (LVSD). This study assesses the prognostic role of strain analysis in RA.</p><p><strong>Methods and results: </strong>Prospective study of 277 RA patients without known heart disease and preserved EF, categorized by left ventricular global longitudinal strain (GLS): normal GLS (≤ - 18%) vs. subclinical LVSD (> - 18%). Primary outcome was a composite of myocardial infarction, HF hospitalization, stroke, or cardiovascular death (MACE). Mean age was 57 years, 79% female. Although mean GLS was within normal (- 20 ± 3%), subclinical LVSD was observed in 24% of patients (n = 67) and was positively correlated with older age (OR 1.54 per 10 years; p < 0.001) and comorbid conditions, such as dyslipidemia (OR 2.27; p = 0.004), obesity (OR 2.29; p = 0.015), and chronic kidney disease (OR 8.39; p = 0.012). Subclinical LVSD was independently associated with a 3.9-fold higher risk of MACE (p = 0.003) and a 3.4-fold higher risk of HF hospitalization/cardiovascular death (p = 0.041). A GLS threshold of > - 18.5% provided optimal sensitivity (78%) and specificity (74%) in identifying patients at elevated MACE risk (AUC = 0.78; p < 0.001).</p><p><strong>Conclusion: </strong>Subclinical LVSD, identified by reduced GLS, was strongly associated with adverse cardiovascular events in RA. Whether these findings have therapeutic implications is worth exploring in clinical trials.</p>","PeriodicalId":10474,"journal":{"name":"Clinical Research in Cardiology","volume":" ","pages":"1191-1203"},"PeriodicalIF":3.7000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12408714/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Research in Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00392-024-02548-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: Patients with rheumatoid arthritis (RA) have an increased risk of cardiac dysfunction and heart failure (HF) due to a pro-inflammatory state. Detecting cardiac dysfunction in RA is challenging as these patients often present preserved ejection fraction (EF) but may have subclinical ventricular dysfunction. Echocardiographic strain analysis is a promising tool for early detection of subclinical left ventricular systolic dysfunction (LVSD). This study assesses the prognostic role of strain analysis in RA.
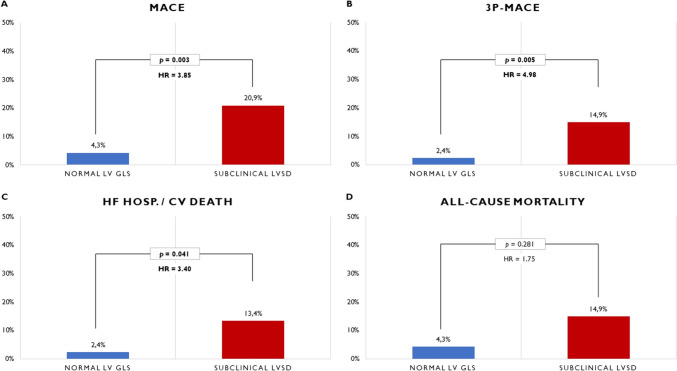
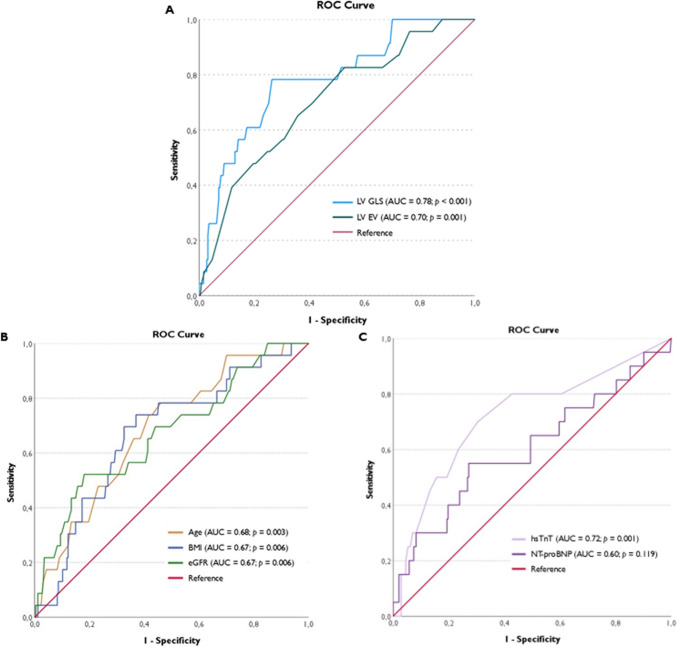
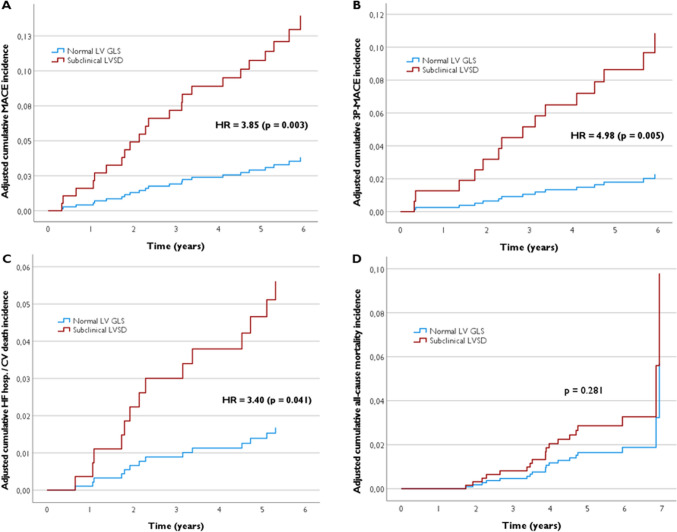
Methods and results: Prospective study of 277 RA patients without known heart disease and preserved EF, categorized by left ventricular global longitudinal strain (GLS): normal GLS (≤ - 18%) vs. subclinical LVSD (> - 18%). Primary outcome was a composite of myocardial infarction, HF hospitalization, stroke, or cardiovascular death (MACE). Mean age was 57 years, 79% female. Although mean GLS was within normal (- 20 ± 3%), subclinical LVSD was observed in 24% of patients (n = 67) and was positively correlated with older age (OR 1.54 per 10 years; p < 0.001) and comorbid conditions, such as dyslipidemia (OR 2.27; p = 0.004), obesity (OR 2.29; p = 0.015), and chronic kidney disease (OR 8.39; p = 0.012). Subclinical LVSD was independently associated with a 3.9-fold higher risk of MACE (p = 0.003) and a 3.4-fold higher risk of HF hospitalization/cardiovascular death (p = 0.041). A GLS threshold of > - 18.5% provided optimal sensitivity (78%) and specificity (74%) in identifying patients at elevated MACE risk (AUC = 0.78; p < 0.001).
Conclusion: Subclinical LVSD, identified by reduced GLS, was strongly associated with adverse cardiovascular events in RA. Whether these findings have therapeutic implications is worth exploring in clinical trials.
期刊介绍:
Clinical Research in Cardiology is an international journal for clinical cardiovascular research. It provides a forum for original and review articles as well as critical perspective articles. Articles are only accepted if they meet stringent scientific standards and have undergone peer review. The journal regularly receives articles from the field of clinical cardiology, angiology, as well as heart and vascular surgery.
As the official journal of the German Cardiac Society, it gives a current and competent survey on the diagnosis and therapy of heart and vascular diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


