Mohammed Abdel-Rassoul, Galal El Shorbagy, Sameh Kotb, Ahmed Alagha, Samih Zamel, Ahmed M Rammah
{"title":"Management of urethral complications after total phallic reconstruction: a single center experience.","authors":"Mohammed Abdel-Rassoul, Galal El Shorbagy, Sameh Kotb, Ahmed Alagha, Samih Zamel, Ahmed M Rammah","doi":"10.5173/ceju.2023.160","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The aim of this study was to evaluate the outcomes of different urethroplasty procedures as well as two novel techniques, invented in our center, in management of urethral complications after total phallic reconstruction.</p><p><strong>Material and methods: </strong>Different urethroplasty procedures were conducted according to the urethral pathology for 36 cis-male patients with urethral complications after total phallic reconstruction including meatoplasty, visual internal urethrotomy, staged Johanson urethroplasty utilizing either buccal mucosal graft or skin graft (Tiersche-Duplay principle), non-transecting urethroplasty (Hieneke-Miiklulicz principle), excision and primary anastomosis, as well as two novel techniques: urethral closure under a suprapubic tunnel and abdominal pedicled skin flap urethroplasty. Each patient was routinely evaluated one month after surgery and every 3 months for 12 months, with clinical evaluation, uroflowmetry and post-void residual urine.</p><p><strong>Results: </strong>With a total of 41 procedures for the 36 patients, 32 patients (88.8 %) could eventually void while standing. The success rate was highest for staged Johanson urethroplasty using split thickness skin graft, staged abdominal pedicled skin flap and excision and primary anastomosis, respectively, while it was lowest for visual internal urethrotomy (0% success) and non-transecting anastomotic urethroplasty (50% success). For staged versus one-stage procedures prospective analysis, 17 out of 26 one-stage procedures (65.4%) succeeded while 13 out of 15 staged procedures (86.6%) succeeded.</p><p><strong>Conclusions: </strong>Urethral complications following phalloplasty require complex procedures demanding a high level of surgical expertise. Abdominal pedicled skin flap urethroplasty is a viable option for long and recalcitrant urethral strictures.</p>","PeriodicalId":9744,"journal":{"name":"Central European Journal of Urology","volume":"77 2","pages":"310-319"},"PeriodicalIF":1.9000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11428358/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Central European Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5173/ceju.2023.160","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/15 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The aim of this study was to evaluate the outcomes of different urethroplasty procedures as well as two novel techniques, invented in our center, in management of urethral complications after total phallic reconstruction.
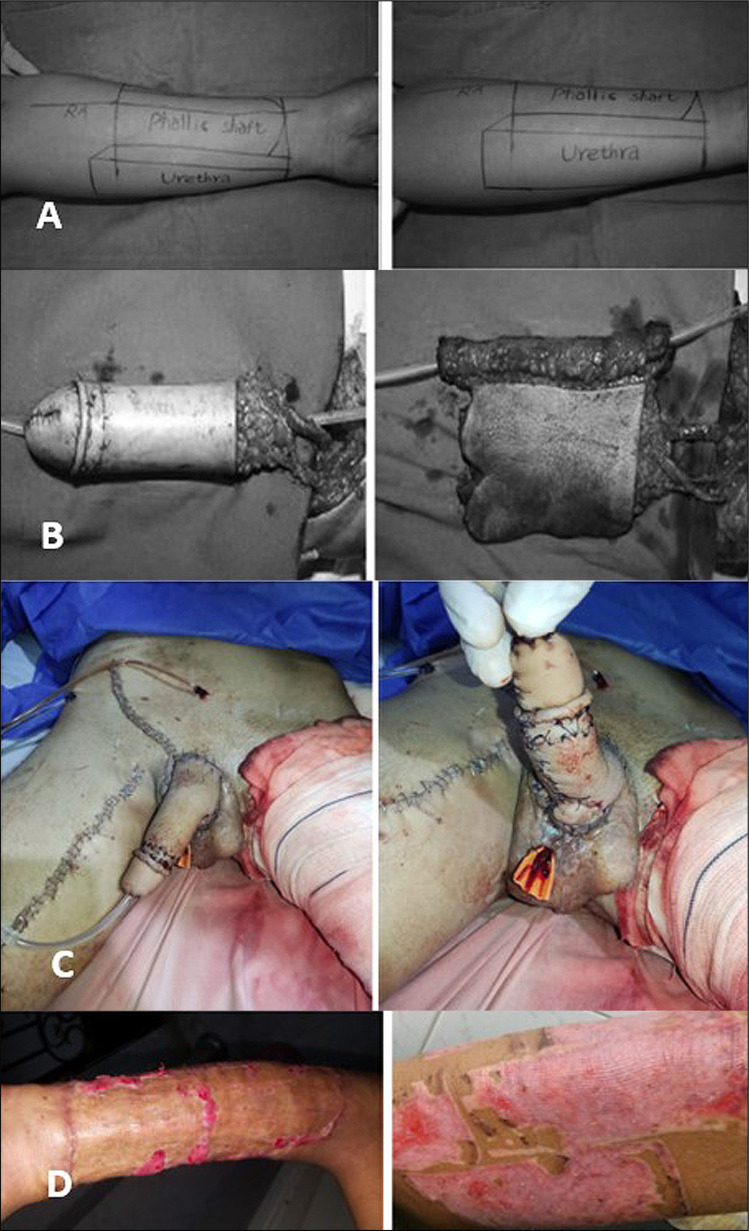
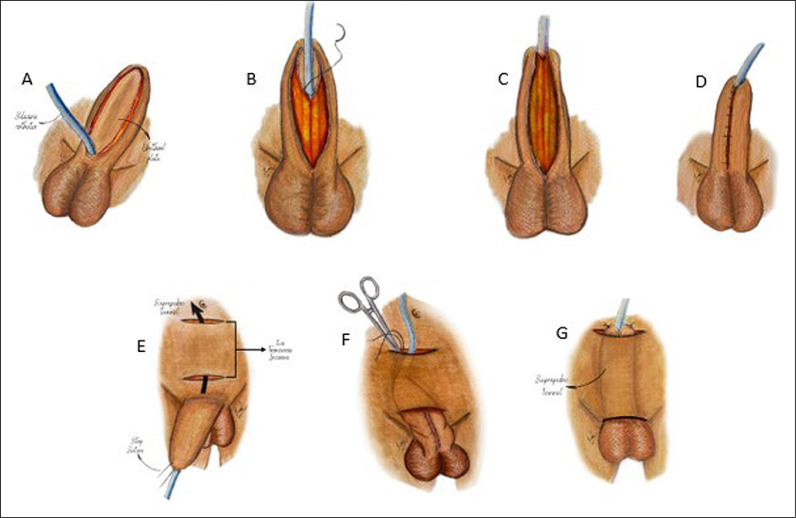
Material and methods: Different urethroplasty procedures were conducted according to the urethral pathology for 36 cis-male patients with urethral complications after total phallic reconstruction including meatoplasty, visual internal urethrotomy, staged Johanson urethroplasty utilizing either buccal mucosal graft or skin graft (Tiersche-Duplay principle), non-transecting urethroplasty (Hieneke-Miiklulicz principle), excision and primary anastomosis, as well as two novel techniques: urethral closure under a suprapubic tunnel and abdominal pedicled skin flap urethroplasty. Each patient was routinely evaluated one month after surgery and every 3 months for 12 months, with clinical evaluation, uroflowmetry and post-void residual urine.
Results: With a total of 41 procedures for the 36 patients, 32 patients (88.8 %) could eventually void while standing. The success rate was highest for staged Johanson urethroplasty using split thickness skin graft, staged abdominal pedicled skin flap and excision and primary anastomosis, respectively, while it was lowest for visual internal urethrotomy (0% success) and non-transecting anastomotic urethroplasty (50% success). For staged versus one-stage procedures prospective analysis, 17 out of 26 one-stage procedures (65.4%) succeeded while 13 out of 15 staged procedures (86.6%) succeeded.
Conclusions: Urethral complications following phalloplasty require complex procedures demanding a high level of surgical expertise. Abdominal pedicled skin flap urethroplasty is a viable option for long and recalcitrant urethral strictures.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


