{"title":"Clinical challenges in early pregnancy in Japan: An update on gestational diabetes","authors":"Takashi Sugiyama, Maki Kawasaki, Naoko Arata","doi":"10.1111/jdi.14319","DOIUrl":null,"url":null,"abstract":"<p>The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study<span><sup>1</sup></span> and subsequently follow-up studies<span><sup>2-4</sup></span> have reported that gestational diabetes mellitus (GDM) is associated with various adverse pregnancy outcomes, which increases the mother's susceptibility to developing type 2 diabetes, and the child's susceptibility to developing obesity and impaired glucose tolerance in the future<span><sup>3-5</sup></span>.</p><p>GDM is diagnosed based on the presence of at least one of the following criteria: pre-load, 1- and 2-h values of the 75-g oral glucose tolerance test (75-g OGTT) of 92, 180 and 153 mg/dL, respectively, at 24–28 weeks' gestation<span><sup>6</sup></span>. These cutoff values were established and recommended by the International Association of Diabetes and Pregnancy Study Groups (IADPSG)<span><sup>6</sup></span>, based on the results of the HAPO study<span><sup>1</sup></span>.</p><p>The diagnostic criteria in Japan are the same as those of the IADPSG<span><sup>7</sup></span>. Although Japan did not participate in the HAPO study, a separate Japanese epidemiological study showed that GDM diagnosed during the second half of pregnancy using these diagnostic criteria was associated with a significantly higher risk of premature birth (<37 weeks), birthweight >90th percentile, hypertensive disorders of pregnancy and cesarean section<span><sup>8</sup></span>. These findings show that the perinatal prognosis of GDM in the second half of pregnancy, as defined by these diagnostic criteria, is poor among Japanese women. Furthermore, Japan uses similar diagnostic cutoff values as the GDM diagnostic criteria in the first half of pregnancy as in the second half of pregnancy. This policy has led to an increase in the incidence of GDM in Japan, as well as other countries<span><sup>8, 9</sup></span>. Incidentally, one study on the prognosis of GDM in the first half of pregnancy in Japan reported that women diagnosed with GDM during the first half of pregnancy had a higher incidence of pre-eclampsia and cesarean section<span><sup>10</sup></span>. We also previously showed that a GDM diagnosis in early pregnancy was associated with adverse pregnancy outcomes compared with a GDM diagnosis in late pregnancy using a previous diagnostic criteria in Japan<span><sup>11</sup></span>. Indeed, it should also be noted that Australia, USA and the UK do not apply these criteria for GDM during early pregnancy so far.</p><p>An important point is that the HAPO study, which formed the basis of the diagnostic criteria for GDM, was based on the 75-g OGTT from 24 to 32 weeks of pregnancy, and not on the blood glucose levels identified during 75-g OGTT in the first half of pregnancy. Indeed, our research has shown that blood glucose levels during 75-g OGTT differ between early and late pregnancy<span><sup>12</sup></span>. As such, the diagnostic criteria for GDM during early pregnancy based on epidemiological and clinical studies should be considered.</p><p>Although the diagnostic criteria for GDM differ, several randomized controlled trials (RCTs) have provided evidence of improved perinatal outcomes of GDM in the second half of pregnancy. One such example is the Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial. In that RCT, 75-g OGTT was carried out between 24 and 34 weeks of pregnancy, with GDM defined as a preloading value of <140 mg/dL and a 2-h loading value between 140 and 198 mg/dL. In the GDM cases in ACHOIS, the intervention group had a significantly lower risk of neonatal complications than the non-intervention group<span><sup>13</sup></span>. However, that RCT study was not based on the IADPSG criteria for GDM. A retrospective cohort study showed that GDM based on IADPSG criteria was associated with improved pregnancy outcomes, although it increases the incidence of GDM<span><sup>14</sup></span>.</p><p>In contrast, one report showed the effectiveness of treatment for GDM in the first half of pregnancy. The Treatment of Booking GDM (TOBOGM) study was an RCT carried out at 17 hospitals enrolling women during their first half of pregnancy<span><sup>15</sup></span>. In that RCT, pregnant women with risk factors for GDM underwent a 75-g OGTT at 4–19 weeks of gestation. Consequently, early GDM was diagnosed in women who met any one of the following criteria (preload value ≥92 mg/dL, 1-h loading value ≥180 mg/dL, 2-h loading value ≥153 mg/dL). The TOBOGM study outcomes included adverse neonatal events, hypertensive disorders of pregnancy and neonatal lean body mass<span><sup>15</sup></span>. In individuals with GDM in the first half of pregnancy, the intervention group had a significantly reduced risk of adverse neonatal events compared with the control group. Furthermore, no statistically significant differences were observed between hypertensive disorders of pregnancy and neonatal lean body mass.</p><p>In the TOBOGM study, a subgroup analysis that classified first-half GDM with a 75-g OGTT value was carried out<span><sup>15</sup></span>. In the HAPO study, the odds ratio for infant birth weight >90th percentile, umbilical cord blood C-peptide >90th percentile and infant body fat mass >90th percentile was 1.75 for 75-g OGTT pre-loading values of 92 mg/dL, 1-h loading values of 180 mg/dL and 2-h loading values of 153 mg/dL. Furthermore, the respective values with odds ratios of 2.00 for 75-g OGTT were 95 mg/dL pre-loading, 191 mg/dL at 1-h and 162 mg/dL at 2-h. The investigators defined patients who met any one of the 95, 191 or 162 mg/dL limits as the high-threshold group, whereas patients who did not meet these values were classified as the low-threshold group, allowing a comparison study. When the outcome was birthweight, no significant association was found between the high-threshold group's intervention and the risk of large for gestational age or small for gestational age in infants. In contrast, the low-threshold group's intervention reduced the risk in large for gestational age infants, but increased the risk in small for gestational age infants. These differences are presumed to reflect infant malnutrition caused by the intervention. Furthermore, a secondary analysis of the TOBOGM study showed that adverse perinatal outcomes were increased with GDM diagnosed during the first half of pregnancy, despite treatment from 24 to 28 weeks' gestation, compared with GDM diagnosed during the second half of pregnancy<span><sup>16</sup></span>. This report suggests that GDM in early pregnancy should be treated. As aforementioned, the diagnostic criteria for GDM in the first half of pregnancy used in the TOBOGM study were the same as those used in Japan; as such, these findings could be considered useful. However, it should be noted that many of the women who were studied met the Japanese definition of obesity in the TOBOGM study.</p><p>The perinatal prognosis of GDM is poor, in both the second and first halves of pregnancy. Although there is evidence that intervention in GDM in the second half of pregnancy improves perinatal prognosis, there is little direct evidence for GDM strictly defined as pre-loading value ≥92 mg/dL, 1-h loading value ≥180 mg/dL and 2-h loading value ≥153 mg/dL; as such, further intervention studies are essential in Japan. One registry study termed the Diabetes and Pregnancy Outcome for Mother and Baby study is currently underway in Japan<span><sup>17</sup></span>, and further analysis results are awaited (Figure 1).</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: N/A.</p><p>Informed consent: N/A.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal studies: N/A.</p>","PeriodicalId":51250,"journal":{"name":"Journal of Diabetes Investigation","volume":"15 12","pages":"1729-1731"},"PeriodicalIF":3.1000,"publicationDate":"2024-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jdi.14319","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Diabetes Investigation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jdi.14319","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study1 and subsequently follow-up studies2-4 have reported that gestational diabetes mellitus (GDM) is associated with various adverse pregnancy outcomes, which increases the mother's susceptibility to developing type 2 diabetes, and the child's susceptibility to developing obesity and impaired glucose tolerance in the future3-5.
GDM is diagnosed based on the presence of at least one of the following criteria: pre-load, 1- and 2-h values of the 75-g oral glucose tolerance test (75-g OGTT) of 92, 180 and 153 mg/dL, respectively, at 24–28 weeks' gestation6. These cutoff values were established and recommended by the International Association of Diabetes and Pregnancy Study Groups (IADPSG)6, based on the results of the HAPO study1.
The diagnostic criteria in Japan are the same as those of the IADPSG7. Although Japan did not participate in the HAPO study, a separate Japanese epidemiological study showed that GDM diagnosed during the second half of pregnancy using these diagnostic criteria was associated with a significantly higher risk of premature birth (<37 weeks), birthweight >90th percentile, hypertensive disorders of pregnancy and cesarean section8. These findings show that the perinatal prognosis of GDM in the second half of pregnancy, as defined by these diagnostic criteria, is poor among Japanese women. Furthermore, Japan uses similar diagnostic cutoff values as the GDM diagnostic criteria in the first half of pregnancy as in the second half of pregnancy. This policy has led to an increase in the incidence of GDM in Japan, as well as other countries8, 9. Incidentally, one study on the prognosis of GDM in the first half of pregnancy in Japan reported that women diagnosed with GDM during the first half of pregnancy had a higher incidence of pre-eclampsia and cesarean section10. We also previously showed that a GDM diagnosis in early pregnancy was associated with adverse pregnancy outcomes compared with a GDM diagnosis in late pregnancy using a previous diagnostic criteria in Japan11. Indeed, it should also be noted that Australia, USA and the UK do not apply these criteria for GDM during early pregnancy so far.
An important point is that the HAPO study, which formed the basis of the diagnostic criteria for GDM, was based on the 75-g OGTT from 24 to 32 weeks of pregnancy, and not on the blood glucose levels identified during 75-g OGTT in the first half of pregnancy. Indeed, our research has shown that blood glucose levels during 75-g OGTT differ between early and late pregnancy12. As such, the diagnostic criteria for GDM during early pregnancy based on epidemiological and clinical studies should be considered.
Although the diagnostic criteria for GDM differ, several randomized controlled trials (RCTs) have provided evidence of improved perinatal outcomes of GDM in the second half of pregnancy. One such example is the Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial. In that RCT, 75-g OGTT was carried out between 24 and 34 weeks of pregnancy, with GDM defined as a preloading value of <140 mg/dL and a 2-h loading value between 140 and 198 mg/dL. In the GDM cases in ACHOIS, the intervention group had a significantly lower risk of neonatal complications than the non-intervention group13. However, that RCT study was not based on the IADPSG criteria for GDM. A retrospective cohort study showed that GDM based on IADPSG criteria was associated with improved pregnancy outcomes, although it increases the incidence of GDM14.
In contrast, one report showed the effectiveness of treatment for GDM in the first half of pregnancy. The Treatment of Booking GDM (TOBOGM) study was an RCT carried out at 17 hospitals enrolling women during their first half of pregnancy15. In that RCT, pregnant women with risk factors for GDM underwent a 75-g OGTT at 4–19 weeks of gestation. Consequently, early GDM was diagnosed in women who met any one of the following criteria (preload value ≥92 mg/dL, 1-h loading value ≥180 mg/dL, 2-h loading value ≥153 mg/dL). The TOBOGM study outcomes included adverse neonatal events, hypertensive disorders of pregnancy and neonatal lean body mass15. In individuals with GDM in the first half of pregnancy, the intervention group had a significantly reduced risk of adverse neonatal events compared with the control group. Furthermore, no statistically significant differences were observed between hypertensive disorders of pregnancy and neonatal lean body mass.
In the TOBOGM study, a subgroup analysis that classified first-half GDM with a 75-g OGTT value was carried out15. In the HAPO study, the odds ratio for infant birth weight >90th percentile, umbilical cord blood C-peptide >90th percentile and infant body fat mass >90th percentile was 1.75 for 75-g OGTT pre-loading values of 92 mg/dL, 1-h loading values of 180 mg/dL and 2-h loading values of 153 mg/dL. Furthermore, the respective values with odds ratios of 2.00 for 75-g OGTT were 95 mg/dL pre-loading, 191 mg/dL at 1-h and 162 mg/dL at 2-h. The investigators defined patients who met any one of the 95, 191 or 162 mg/dL limits as the high-threshold group, whereas patients who did not meet these values were classified as the low-threshold group, allowing a comparison study. When the outcome was birthweight, no significant association was found between the high-threshold group's intervention and the risk of large for gestational age or small for gestational age in infants. In contrast, the low-threshold group's intervention reduced the risk in large for gestational age infants, but increased the risk in small for gestational age infants. These differences are presumed to reflect infant malnutrition caused by the intervention. Furthermore, a secondary analysis of the TOBOGM study showed that adverse perinatal outcomes were increased with GDM diagnosed during the first half of pregnancy, despite treatment from 24 to 28 weeks' gestation, compared with GDM diagnosed during the second half of pregnancy16. This report suggests that GDM in early pregnancy should be treated. As aforementioned, the diagnostic criteria for GDM in the first half of pregnancy used in the TOBOGM study were the same as those used in Japan; as such, these findings could be considered useful. However, it should be noted that many of the women who were studied met the Japanese definition of obesity in the TOBOGM study.
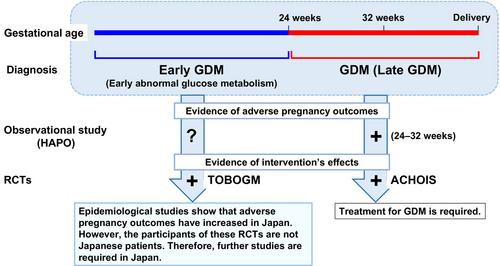
The perinatal prognosis of GDM is poor, in both the second and first halves of pregnancy. Although there is evidence that intervention in GDM in the second half of pregnancy improves perinatal prognosis, there is little direct evidence for GDM strictly defined as pre-loading value ≥92 mg/dL, 1-h loading value ≥180 mg/dL and 2-h loading value ≥153 mg/dL; as such, further intervention studies are essential in Japan. One registry study termed the Diabetes and Pregnancy Outcome for Mother and Baby study is currently underway in Japan17, and further analysis results are awaited (Figure 1).
The authors declare no conflict of interest.
Approval of the research protocol: N/A.
Informed consent: N/A.
Registry and the registration no. of the study/trial: N/A.
期刊介绍:
Journal of Diabetes Investigation is your core diabetes journal from Asia; the official journal of the Asian Association for the Study of Diabetes (AASD). The journal publishes original research, country reports, commentaries, reviews, mini-reviews, case reports, letters, as well as editorials and news. Embracing clinical and experimental research in diabetes and related areas, the Journal of Diabetes Investigation includes aspects of prevention, treatment, as well as molecular aspects and pathophysiology. Translational research focused on the exchange of ideas between clinicians and researchers is also welcome. Journal of Diabetes Investigation is indexed by Science Citation Index Expanded (SCIE).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


