{"title":"Prognostic Implications of Timing of Immunotherapy in Stage IV Non-Small Cell Lung Cancer.","authors":"Jorge Raul Vazquez-Urrutia, Max Greenberg, Junjia Zhu, Shinkichi Takamori, Takefumi Komiya","doi":"10.14740/wjon1924","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Currently, the established approach for addressing stage IV non-small cell lung cancer (NSCLC) involves combining chemotherapy with immunotherapy. However, the necessity for molecular analysis prior to commencing immunotherapy often results in a delay in its initiation following the commencement of chemotherapy. Therefore, this study aimed to study the significance of postponing immunotherapy on pertinent patient outcomes.</p><p><strong>Methods: </strong>Using the National Cancer Database (NCBD), patients diagnosed with stage IV NSCLC between 2017 and 2018 were screened. Inclusion criteria comprised those treated with multi-agent chemotherapy as the first-line therapy within 30 days of treatment, surviving beyond 2 months of diagnosis, and absence of neuroendocrine pathology. Patients were grouped among those receiving immunotherapy within 30 days of chemotherapy, immunotherapy within 31 - 60 days of chemotherapy, or chemotherapy alone. Clinical characteristics were collected and their correlation with the timing of immunotherapy was evaluated. The impact of delaying immunotherapy on overall survival (OS) was investigated using Kaplan-Meier analysis. Multivariate Cox regression analysis was employed to identify independent prognostic variables associated with OS.</p><p><strong>Results: </strong>Our cohort comprised 99,008 patients with clinical stage IV NSCLC diagnosed between 2017 and 2018, which were distributed in the three treatment groups described above. Patients receiving immunotherapy within 30 days of chemotherapy showed greater OS in contrast to both those subjected to delayed immunotherapy (hazard ratio (HR) = 0.74, 95% confidence interval (CI): 0.64 - 0.87, P = 0.0003). Subsequent multivariate regression analysis showed that postponing immunotherapy, older age, male sex, white race, non-adenocarcinoma histology, higher clinical N stage, use of radiation treatment, and presence of liver metastasis were all associated with worse OS.</p><p><strong>Conclusions: </strong>Introducing immunotherapy within the first 30 days of chemotherapy initiation significantly increases survival in patients with stage IV NSCLC.</p>","PeriodicalId":46797,"journal":{"name":"World Journal of Oncology","volume":"15 5","pages":"769-776"},"PeriodicalIF":2.2000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11424121/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/wjon1924","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Currently, the established approach for addressing stage IV non-small cell lung cancer (NSCLC) involves combining chemotherapy with immunotherapy. However, the necessity for molecular analysis prior to commencing immunotherapy often results in a delay in its initiation following the commencement of chemotherapy. Therefore, this study aimed to study the significance of postponing immunotherapy on pertinent patient outcomes.
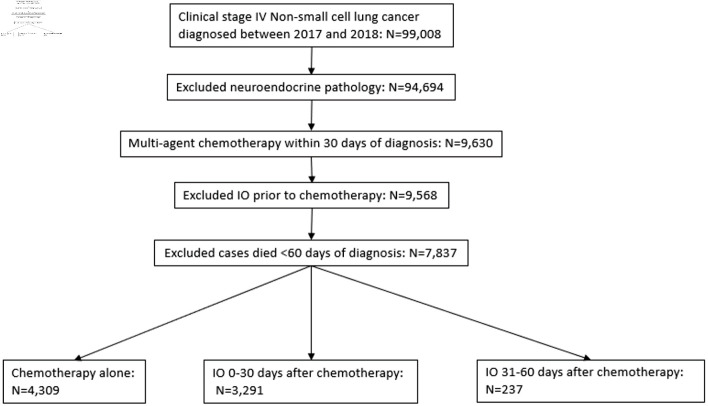
Methods: Using the National Cancer Database (NCBD), patients diagnosed with stage IV NSCLC between 2017 and 2018 were screened. Inclusion criteria comprised those treated with multi-agent chemotherapy as the first-line therapy within 30 days of treatment, surviving beyond 2 months of diagnosis, and absence of neuroendocrine pathology. Patients were grouped among those receiving immunotherapy within 30 days of chemotherapy, immunotherapy within 31 - 60 days of chemotherapy, or chemotherapy alone. Clinical characteristics were collected and their correlation with the timing of immunotherapy was evaluated. The impact of delaying immunotherapy on overall survival (OS) was investigated using Kaplan-Meier analysis. Multivariate Cox regression analysis was employed to identify independent prognostic variables associated with OS.
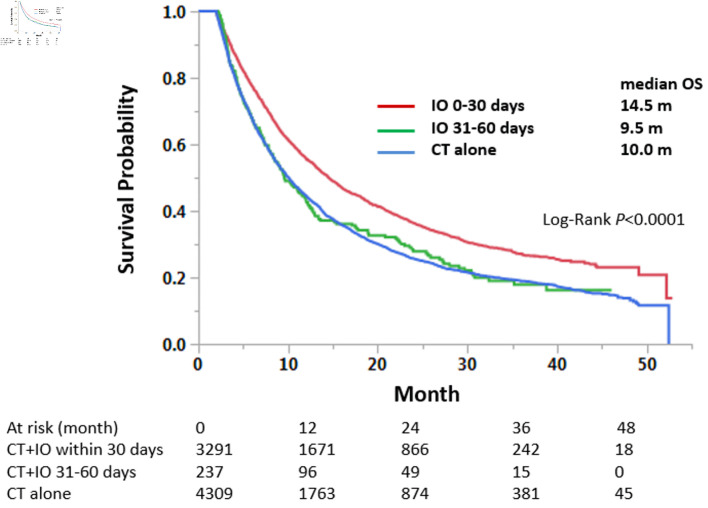
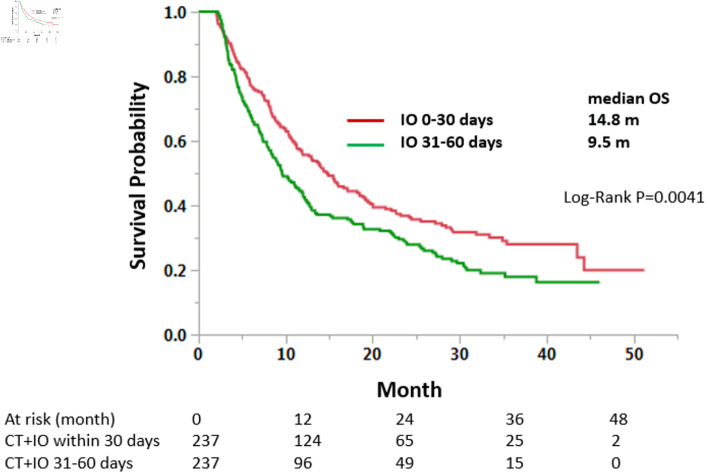
Results: Our cohort comprised 99,008 patients with clinical stage IV NSCLC diagnosed between 2017 and 2018, which were distributed in the three treatment groups described above. Patients receiving immunotherapy within 30 days of chemotherapy showed greater OS in contrast to both those subjected to delayed immunotherapy (hazard ratio (HR) = 0.74, 95% confidence interval (CI): 0.64 - 0.87, P = 0.0003). Subsequent multivariate regression analysis showed that postponing immunotherapy, older age, male sex, white race, non-adenocarcinoma histology, higher clinical N stage, use of radiation treatment, and presence of liver metastasis were all associated with worse OS.
Conclusions: Introducing immunotherapy within the first 30 days of chemotherapy initiation significantly increases survival in patients with stage IV NSCLC.
期刊介绍:
World Journal of Oncology, bimonthly, publishes original contributions describing basic research and clinical investigation of cancer, on the cellular, molecular, prevention, diagnosis, therapy and prognosis aspects. The submissions can be basic research or clinical investigation oriented. This journal welcomes those submissions focused on the clinical trials of new treatment modalities for cancer, and those submissions focused on molecular or cellular research of the oncology pathogenesis. Case reports submitted for consideration of publication should explore either a novel genomic event/description or a new safety signal from an oncolytic agent. The areas of interested manuscripts are these disciplines: tumor immunology and immunotherapy; cancer molecular pharmacology and chemotherapy; drug sensitivity and resistance; cancer epidemiology; clinical trials; cancer pathology; radiobiology and radiation oncology; solid tumor oncology; hematological malignancies; surgical oncology; pediatric oncology; molecular oncology and cancer genes; gene therapy; cancer endocrinology; cancer metastasis; prevention and diagnosis of cancer; other cancer related subjects. The types of manuscripts accepted are original article, review, editorial, short communication, case report, letter to the editor, book review.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


