Wallace Bourgeois, Jonathan Paolino, Riley Garland, Kevin Campbell, Francesca Alvarez-Calderon, A Lindsay Frazier, Allison F O'Neill, Maya Ilowite, Chris I Wong
{"title":"Outpatient Management of Fever and Neutropenia in Low-risk Children with Solid Tumors: A Quality Improvement Initiative.","authors":"Wallace Bourgeois, Jonathan Paolino, Riley Garland, Kevin Campbell, Francesca Alvarez-Calderon, A Lindsay Frazier, Allison F O'Neill, Maya Ilowite, Chris I Wong","doi":"10.1097/pq9.0000000000000771","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Management of febrile neutropenia in pediatric oncology usually requires inpatient parenteral antibiotics after initial evaluation, but some patients at lower risk of sepsis could be safely managed outpatient. We describe a quality improvement project to increase outpatient management of fever and neutropenia.</p><p><strong>Methods: </strong>We designed a standardized algorithm for children with a solid tumor diagnosis and low risk for bacteremia. The aim was to achieve outpatient management for at least 80% of eligible patients within 20 months of project initiation. We used plan-do-study-act cycles to improve algorithm compliance, including optimizing medical record decision support, developing targeted educational materials and outreach, and restructuring outpatient processes to allow for close follow-up. We surveyed patients (age ≥12 y) and parents/caregivers to assess the impact of outpatient management.</p><p><strong>Results: </strong>The initiative led to 71% (n = 34) of eligible patients being managed as outpatients. Six percent (n = 2) of patients developed bacteremia, resulting in hospital admission. Fifteen of 26 parents/caregivers and five of 11 patients approached completed the survey. For the preferred setting of febrile neutropenia management, 83% of patients preferred to be home versus 40% of parents/caregivers. No patient expressed any of the three highest ratings in the question exploring fear regarding outpatient febrile neutropenia management versus 67% of parents/caregivers.</p><p><strong>Conclusions: </strong>Some children with a solid tumor diagnosis at low risk for bacteremia are safely managed for febrile neutropenia as outpatients. Targeted efforts to engage parents/caregivers early in this practice change are necessary for success.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 5","pages":"e771"},"PeriodicalIF":1.1000,"publicationDate":"2024-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11424129/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000771","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Management of febrile neutropenia in pediatric oncology usually requires inpatient parenteral antibiotics after initial evaluation, but some patients at lower risk of sepsis could be safely managed outpatient. We describe a quality improvement project to increase outpatient management of fever and neutropenia.
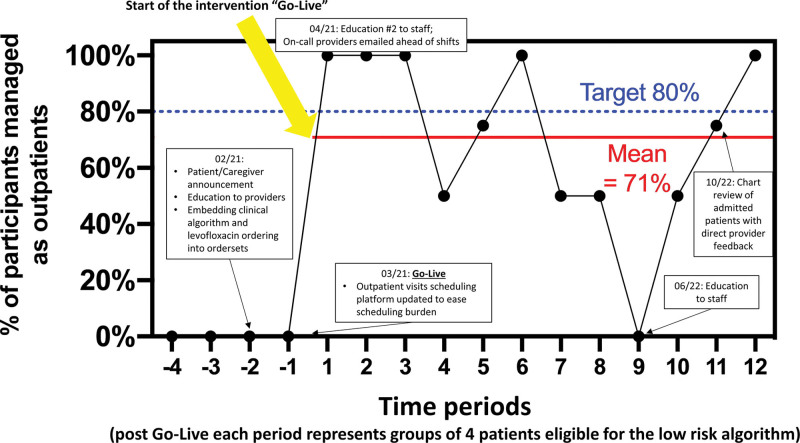
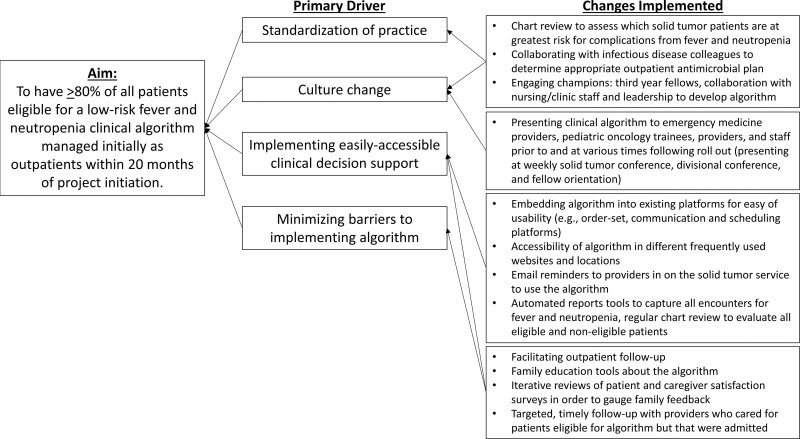
Methods: We designed a standardized algorithm for children with a solid tumor diagnosis and low risk for bacteremia. The aim was to achieve outpatient management for at least 80% of eligible patients within 20 months of project initiation. We used plan-do-study-act cycles to improve algorithm compliance, including optimizing medical record decision support, developing targeted educational materials and outreach, and restructuring outpatient processes to allow for close follow-up. We surveyed patients (age ≥12 y) and parents/caregivers to assess the impact of outpatient management.
Results: The initiative led to 71% (n = 34) of eligible patients being managed as outpatients. Six percent (n = 2) of patients developed bacteremia, resulting in hospital admission. Fifteen of 26 parents/caregivers and five of 11 patients approached completed the survey. For the preferred setting of febrile neutropenia management, 83% of patients preferred to be home versus 40% of parents/caregivers. No patient expressed any of the three highest ratings in the question exploring fear regarding outpatient febrile neutropenia management versus 67% of parents/caregivers.
Conclusions: Some children with a solid tumor diagnosis at low risk for bacteremia are safely managed for febrile neutropenia as outpatients. Targeted efforts to engage parents/caregivers early in this practice change are necessary for success.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


