Shuo Wang, Zexi Rao, Rui Cao, Anne H Blaes, Josef Coresh, Rajat Deo, Ruth Dubin, Corinne E Joshu, Benoit Lehallier, Pamela L Lutsey, James S Pankow, Wendy S Post, Jerome I Rotter, Sanaz Sedaghat, Weihong Tang, Bharat Thyagarajan, Keenan A Walker, Peter Ganz, Elizabeth A Platz, Weihua Guan, Anna Prizment
{"title":"Development, characterization, and replication of proteomic aging clocks: Analysis of 2 population-based cohorts.","authors":"Shuo Wang, Zexi Rao, Rui Cao, Anne H Blaes, Josef Coresh, Rajat Deo, Ruth Dubin, Corinne E Joshu, Benoit Lehallier, Pamela L Lutsey, James S Pankow, Wendy S Post, Jerome I Rotter, Sanaz Sedaghat, Weihong Tang, Bharat Thyagarajan, Keenan A Walker, Peter Ganz, Elizabeth A Platz, Weihua Guan, Anna Prizment","doi":"10.1371/journal.pmed.1004464","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Biological age may be estimated by proteomic aging clocks (PACs). Previous published PACs were constructed either in smaller studies or mainly in white individuals, and they used proteomic measures from only one-time point. In this study, we created de novo PACs and compared their performance to published PACs at 2 different time points in the Atherosclerosis Risk in Communities (ARIC) study of white and black participants (around 75% white and 25% black).</p><p><strong>Medthods and findings: </strong>A total of 4,712 plasma proteins were measured using SomaScan in blood samples collected in 1990 to 1992 from 11,761 midlife participants (aged 46 to 70 years) and in 2011 to 2013 from 5,183 late-life participants (aged 66 to 90 years). The de novo ARIC PACs were constructed by training them against chronological age using elastic net regression in two-thirds of healthy participants in midlife and late life and validated in the remaining one-third of healthy participants at the corresponding time point. We also computed 3 published PACs. We estimated age acceleration for each PAC as residuals after regressing each PAC on chronological age. We also calculated the change in age acceleration from midlife to late life. We examined the associations of age acceleration and change in age acceleration with mortality through 2019 from all-cause, cardiovascular disease (CVD), cancer, and lower respiratory disease (LRD) using Cox proportional hazards regression in participants (irrespective of health) after excluding the training set. The model was adjusted for chronological age, smoking, body mass index (BMI), and other confounders. We externally validated the midlife PAC using the Multi-Ethnic Study of Atherosclerosis (MESA) Exam 1 data. The ARIC PACs had a slightly stronger correlation with chronological age than published PACs in healthy participants at each time point. Associations with mortality were similar for the ARIC PACs and published PACs. For late-life and midlife age acceleration for the ARIC PACs, respectively, hazard ratios (HRs) per 1 standard deviation were 1.65 and 1.38 (both p < 0.001) for all-cause mortality, 1.37 and 1.20 (both p < 0.001) for CVD mortality, 1.21 (p = 0.028) and 1.04 (p = 0.280) for cancer mortality, and 1.68 and 1.36 (both p < 0.001) for LRD mortality. For the change in age acceleration, HRs for all-cause, CVD, and LRD mortality were comparable to the HRs for late-life age acceleration. The association between the change in age acceleration and cancer mortality was not significant. The external validation of the midlife PAC in MESA showed significant associations with mortality, as observed for midlife participants in ARIC. The main limitation is that our PACs were constructed in midlife and late-life participants. It is unknown whether these PACs could be applied to young individuals.</p><p><strong>Conclusions: </strong>In this longitudinal study, we found that the ARIC PACs and published PACs were similarly associated with an increased risk of mortality. These findings suggested that PACs show promise as biomarkers of biological age. PACs may be serve as tools to predict mortality and evaluate the effect of anti-aging lifestyle and therapeutic interventions.</p>","PeriodicalId":49008,"journal":{"name":"PLoS Medicine","volume":"21 9","pages":"e1004464"},"PeriodicalIF":9.9000,"publicationDate":"2024-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11460707/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1004464","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Biological age may be estimated by proteomic aging clocks (PACs). Previous published PACs were constructed either in smaller studies or mainly in white individuals, and they used proteomic measures from only one-time point. In this study, we created de novo PACs and compared their performance to published PACs at 2 different time points in the Atherosclerosis Risk in Communities (ARIC) study of white and black participants (around 75% white and 25% black).
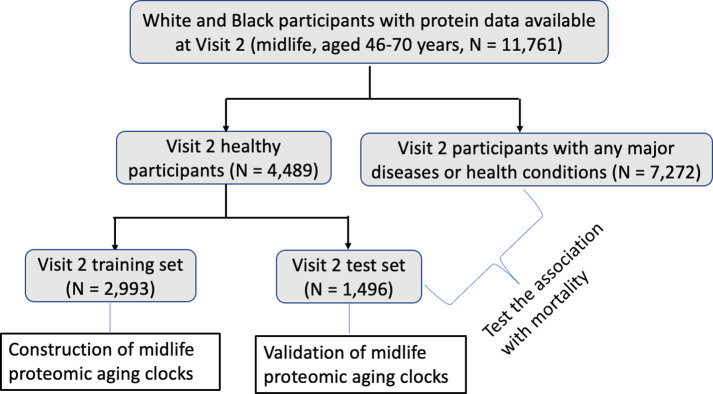
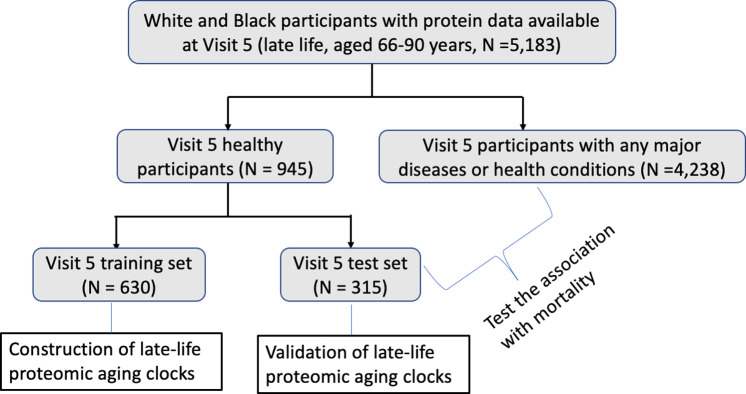
Medthods and findings: A total of 4,712 plasma proteins were measured using SomaScan in blood samples collected in 1990 to 1992 from 11,761 midlife participants (aged 46 to 70 years) and in 2011 to 2013 from 5,183 late-life participants (aged 66 to 90 years). The de novo ARIC PACs were constructed by training them against chronological age using elastic net regression in two-thirds of healthy participants in midlife and late life and validated in the remaining one-third of healthy participants at the corresponding time point. We also computed 3 published PACs. We estimated age acceleration for each PAC as residuals after regressing each PAC on chronological age. We also calculated the change in age acceleration from midlife to late life. We examined the associations of age acceleration and change in age acceleration with mortality through 2019 from all-cause, cardiovascular disease (CVD), cancer, and lower respiratory disease (LRD) using Cox proportional hazards regression in participants (irrespective of health) after excluding the training set. The model was adjusted for chronological age, smoking, body mass index (BMI), and other confounders. We externally validated the midlife PAC using the Multi-Ethnic Study of Atherosclerosis (MESA) Exam 1 data. The ARIC PACs had a slightly stronger correlation with chronological age than published PACs in healthy participants at each time point. Associations with mortality were similar for the ARIC PACs and published PACs. For late-life and midlife age acceleration for the ARIC PACs, respectively, hazard ratios (HRs) per 1 standard deviation were 1.65 and 1.38 (both p < 0.001) for all-cause mortality, 1.37 and 1.20 (both p < 0.001) for CVD mortality, 1.21 (p = 0.028) and 1.04 (p = 0.280) for cancer mortality, and 1.68 and 1.36 (both p < 0.001) for LRD mortality. For the change in age acceleration, HRs for all-cause, CVD, and LRD mortality were comparable to the HRs for late-life age acceleration. The association between the change in age acceleration and cancer mortality was not significant. The external validation of the midlife PAC in MESA showed significant associations with mortality, as observed for midlife participants in ARIC. The main limitation is that our PACs were constructed in midlife and late-life participants. It is unknown whether these PACs could be applied to young individuals.
Conclusions: In this longitudinal study, we found that the ARIC PACs and published PACs were similarly associated with an increased risk of mortality. These findings suggested that PACs show promise as biomarkers of biological age. PACs may be serve as tools to predict mortality and evaluate the effect of anti-aging lifestyle and therapeutic interventions.
期刊介绍:
PLOS Medicine is a prominent platform for discussing and researching global health challenges. The journal covers a wide range of topics, including biomedical, environmental, social, and political factors affecting health. It prioritizes articles that contribute to clinical practice, health policy, or a better understanding of pathophysiology, ultimately aiming to improve health outcomes across different settings.
The journal is unwavering in its commitment to uphold the highest ethical standards in medical publishing. This includes actively managing and disclosing any conflicts of interest related to reporting, reviewing, and publishing. PLOS Medicine promotes transparency in the entire review and publication process. The journal also encourages data sharing and encourages the reuse of published work. Additionally, authors retain copyright for their work, and the publication is made accessible through Open Access with no restrictions on availability and dissemination.
PLOS Medicine takes measures to avoid conflicts of interest associated with advertising drugs and medical devices or engaging in the exclusive sale of reprints.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


