Vinita Bahl, Marc J Moote, Hsou Mei Hu, Darrell A Campbell
{"title":"Impact of Clinical Decision Support with Mandatory versus Voluntary Venous Thromboembolism Risk Assessment in Hospitalized Patients.","authors":"Vinita Bahl, Marc J Moote, Hsou Mei Hu, Darrell A Campbell","doi":"10.1055/s-0044-1790519","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b> Venous thromboembolism (VTE) causes significant preventable morbidity and mortality in hospitalized patients. Assessing VTE risk is essential to initiating appropriate prophylaxis and reducing VTE outcomes. Studies show that computerized clinical decision support (CDS) can improve VTE risk assessment (RA), prophylaxis, and outcomes but few examined the effectiveness of specific design features. From 2008 to 2016, University of Michigan Health implemented CDS for VTE prevention in four stages, which alternated between voluntary and mandatory RA using the 2005 Caprini model and generated inpatient orders for risk-appropriate prophylaxis based on CHEST guidelines. This cross-sectional study evaluated the impact of mandatory versus voluntary RA on VTE prophylaxis and outcomes for adult medical and surgical patients admitted to the health system. <b>Methods</b> Interrupted time series analysis was conducted to evaluate the trend in smart order set-recommended VTE prophylaxis by CDS stage. Logistic regression with CDS stage as the primary independent variable was used in pairwise comparisons of VTE during hospitalization and within 90 days post-discharge for mandatory versus voluntary RA. Adjusted odd ratios (ORs) were calculated for total, in-hospital, and post-discharge VTE. <b>Results</b> In this study of 223,405 inpatients over 8 years, smart order set-recommended prophylaxis increased from 65 to 79%; it increased significantly when voluntary RA in Stage 1 became mandatory in Stage 2 (10.59%, <i>p</i> < 0.001) and decreased significantly when it returned to voluntary in Stage 3 (-11.24%, <i>p</i> < 0.001). The rate increased slightly when mandatory RA was reestablished in Stage 4 (0.23%, <i>p</i> = 0.935). Adjusted ORs for VTE were lower for mandatory RA versus adjacent stages with voluntary RA. The adjusted OR for Stage 2 versus Stage 1 was 14% lower ( <i>p</i> < 0.05) and versus Stage 3 was 11% lower ( <i>p</i> < 0.05). The adjusted OR for Stage 4 versus Stage 3 was 4% lower ( <i>p</i> = 0.60). These results were driven by changes in in-hospital VTE. By contrast, the incidence of post-discharge VTE increased in each successive stage. <b>Conclusion</b> Mandatory RA was more effective in improving smart order set-recommended prophylaxis and VTE outcomes, particularly in-hospital VTE. Post-discharge VTE increased despite high adherence to risk-appropriate prophylaxis, indicating that guidelines for extended, post-discharge prophylaxis are needed to further reduce VTE for hospitalized patients.</p>","PeriodicalId":94220,"journal":{"name":"TH open : companion journal to thrombosis and haemostasis","volume":"8 3","pages":"e317-e328"},"PeriodicalIF":1.8000,"publicationDate":"2024-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11392591/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"TH open : companion journal to thrombosis and haemostasis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1790519","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
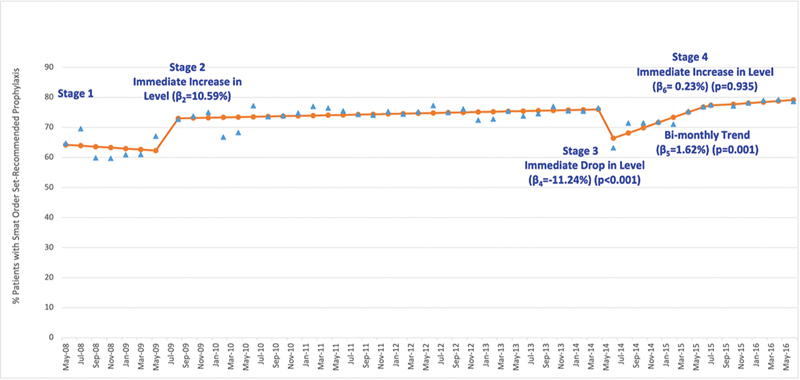
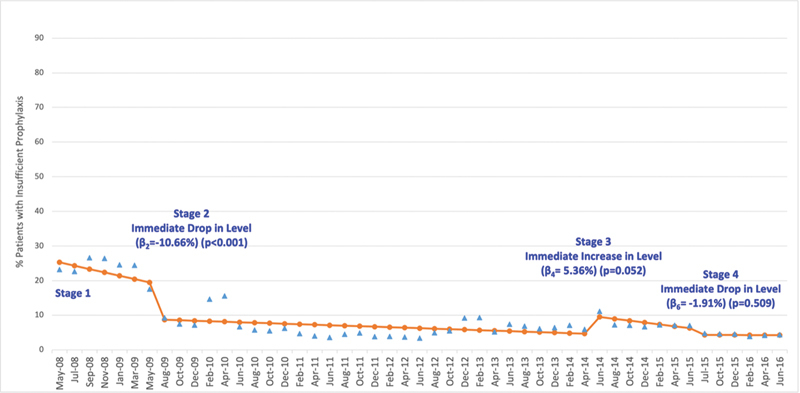
Background Venous thromboembolism (VTE) causes significant preventable morbidity and mortality in hospitalized patients. Assessing VTE risk is essential to initiating appropriate prophylaxis and reducing VTE outcomes. Studies show that computerized clinical decision support (CDS) can improve VTE risk assessment (RA), prophylaxis, and outcomes but few examined the effectiveness of specific design features. From 2008 to 2016, University of Michigan Health implemented CDS for VTE prevention in four stages, which alternated between voluntary and mandatory RA using the 2005 Caprini model and generated inpatient orders for risk-appropriate prophylaxis based on CHEST guidelines. This cross-sectional study evaluated the impact of mandatory versus voluntary RA on VTE prophylaxis and outcomes for adult medical and surgical patients admitted to the health system. Methods Interrupted time series analysis was conducted to evaluate the trend in smart order set-recommended VTE prophylaxis by CDS stage. Logistic regression with CDS stage as the primary independent variable was used in pairwise comparisons of VTE during hospitalization and within 90 days post-discharge for mandatory versus voluntary RA. Adjusted odd ratios (ORs) were calculated for total, in-hospital, and post-discharge VTE. Results In this study of 223,405 inpatients over 8 years, smart order set-recommended prophylaxis increased from 65 to 79%; it increased significantly when voluntary RA in Stage 1 became mandatory in Stage 2 (10.59%, p < 0.001) and decreased significantly when it returned to voluntary in Stage 3 (-11.24%, p < 0.001). The rate increased slightly when mandatory RA was reestablished in Stage 4 (0.23%, p = 0.935). Adjusted ORs for VTE were lower for mandatory RA versus adjacent stages with voluntary RA. The adjusted OR for Stage 2 versus Stage 1 was 14% lower ( p < 0.05) and versus Stage 3 was 11% lower ( p < 0.05). The adjusted OR for Stage 4 versus Stage 3 was 4% lower ( p = 0.60). These results were driven by changes in in-hospital VTE. By contrast, the incidence of post-discharge VTE increased in each successive stage. Conclusion Mandatory RA was more effective in improving smart order set-recommended prophylaxis and VTE outcomes, particularly in-hospital VTE. Post-discharge VTE increased despite high adherence to risk-appropriate prophylaxis, indicating that guidelines for extended, post-discharge prophylaxis are needed to further reduce VTE for hospitalized patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


