Sunil Samnani, Emily C L Wong, Hasan Hamam, Parambir S Dulai, John K Marshall, Vipul Jairath, Walter Reinisch, Neeraj Narula
{"title":"Outcomes of Patients With Prior Biologic Intolerance Are Better Than Those With Biologic Failure in Clinical Trials of Inflammatory Bowel Disease.","authors":"Sunil Samnani, Emily C L Wong, Hasan Hamam, Parambir S Dulai, John K Marshall, Vipul Jairath, Walter Reinisch, Neeraj Narula","doi":"10.1093/ecco-jcc/jjae151","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Inflammatory bowel disease (IBD) trials often stratify patients by prior biologic exposure, including prior biologic failure or intolerance. This study aimed to assess clinical outcomes in IBD patients with prior biologic failure vs intolerance treated with ustekinumab or vedolizumab.</p><p><strong>Methods: </strong>A post-hoc analysis of ulcerative colitis (UC) and Crohn's disease (CD) clinical trials for ustekinumab (UNITI and UNIFI) and vedolizumab (GEMINI-1 and GEMINI-2) was performed. Clinical response, clinical remission, and endoscopic improvement (for UC) were compared among biologic naïve, biologic failure, and biologic intolerant patients. Statistical analyses, including chi-square tests and logistic regression, were performed.</p><p><strong>Results: </strong>A total of 1178 UC and 1439 CD patients received either ustekinumab or vedolizumab. In UC, biologic intolerant patients exhibited higher clinical response (54.7% vs 38.8%, aOR 1.87 [95% CI, 0.93-3.73]), clinical remission (25.0% vs 11.0%, aOR 2.84 [95% CI, 1.47-5.49]), and endoscopic improvement (40.6% vs 24.8%, aOR 2.76 [95% CI, 1.28-5.94]) compared to biologic failure, with outcomes similar to biologic naïve patients. In biologic intolerant CD patients, clinical response was similar between prior biologic failure and intolerance (34.2% vs 32.8%), but after adjustment for potential confounders, biologic intolerance was associated with higher odds of clinical response (aOR: 1.67, 95% CI, 1.09-2.55), with no significant difference observed for clinical remission (aOR: 1.48, 95% CI, 0.88-2.49).</p><p><strong>Conclusions: </strong>Improved treatment outcomes were generally observed in patients with biologic intolerance compared to failure, especially in UC, where outcomes were similar to biologic naïve patients. Future clinical trials should meticulously differentiate prior biologic failure vs intolerance to mitigate potential bias.</p>","PeriodicalId":94074,"journal":{"name":"Journal of Crohn's & colitis","volume":" ","pages":""},"PeriodicalIF":8.7000,"publicationDate":"2025-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11945295/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Crohn's & colitis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ecco-jcc/jjae151","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: Inflammatory bowel disease (IBD) trials often stratify patients by prior biologic exposure, including prior biologic failure or intolerance. This study aimed to assess clinical outcomes in IBD patients with prior biologic failure vs intolerance treated with ustekinumab or vedolizumab.
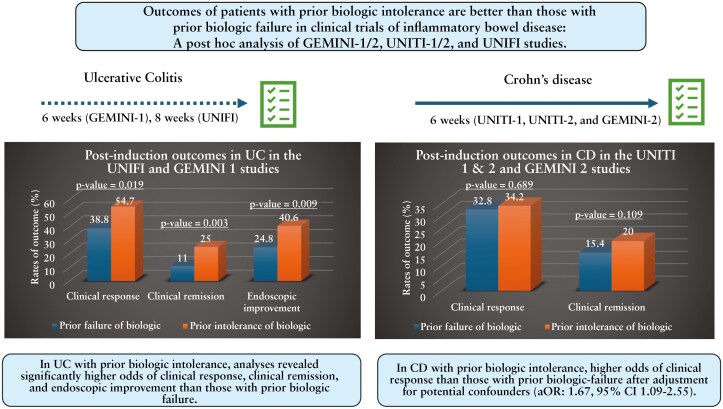
Methods: A post-hoc analysis of ulcerative colitis (UC) and Crohn's disease (CD) clinical trials for ustekinumab (UNITI and UNIFI) and vedolizumab (GEMINI-1 and GEMINI-2) was performed. Clinical response, clinical remission, and endoscopic improvement (for UC) were compared among biologic naïve, biologic failure, and biologic intolerant patients. Statistical analyses, including chi-square tests and logistic regression, were performed.
Results: A total of 1178 UC and 1439 CD patients received either ustekinumab or vedolizumab. In UC, biologic intolerant patients exhibited higher clinical response (54.7% vs 38.8%, aOR 1.87 [95% CI, 0.93-3.73]), clinical remission (25.0% vs 11.0%, aOR 2.84 [95% CI, 1.47-5.49]), and endoscopic improvement (40.6% vs 24.8%, aOR 2.76 [95% CI, 1.28-5.94]) compared to biologic failure, with outcomes similar to biologic naïve patients. In biologic intolerant CD patients, clinical response was similar between prior biologic failure and intolerance (34.2% vs 32.8%), but after adjustment for potential confounders, biologic intolerance was associated with higher odds of clinical response (aOR: 1.67, 95% CI, 1.09-2.55), with no significant difference observed for clinical remission (aOR: 1.48, 95% CI, 0.88-2.49).
Conclusions: Improved treatment outcomes were generally observed in patients with biologic intolerance compared to failure, especially in UC, where outcomes were similar to biologic naïve patients. Future clinical trials should meticulously differentiate prior biologic failure vs intolerance to mitigate potential bias.
背景和目的:炎症性肠病(IBD)试验通常根据患者既往生物制剂暴露情况进行分层,包括既往生物制剂失败或不耐受。本研究旨在评估曾接受过乌司替尼或韦多珠单抗治疗的生物制剂失败或不耐受的IBD患者的临床疗效:对溃疡性结肠炎(UC)和克罗恩病(CD)的乌斯特库单抗(UNITI、UNIFI)和维妥珠单抗(GEMINI-1、GEMINI-2)临床试验进行了事后分析。比较了生物制剂新药患者、生物制剂失败患者和生物制剂不耐受患者的临床反应、临床缓解和内窥镜改善(针对 UC)情况。统计分析包括卡方检验和逻辑回归:结果:1178 名 UC 和 1439 名 CD 患者接受了乌司替尼或韦多珠单抗治疗。在 UC 患者中,与生物治疗失败相比,生物治疗不耐受患者的临床反应(54.7% vs. 38.8%,aOR 1.87 [95% CI 0.93-3.73])、临床缓解(25.0% vs. 11.0%,aOR 2.84 [95% CI 1.47-5.49])和内镜改善(40.6% vs. 24.8%,aOR 2.76 [95% CI 1.28-5.94])更高,结果与生物治疗无效患者相似。在生物制剂不耐受的CD患者中,既往生物制剂失败和不耐受的患者临床应答相似(34.2% vs 32.8%),但在调整潜在混杂因素后,生物制剂不耐受与临床应答几率较高(aOR:1.67,95% CI 1.09-2.55)相关,而临床缓解与之无显著差异(aOR:1.48,95% CI 0.88-2.49):结论:与治疗失败相比,生物制剂不耐受患者的治疗效果普遍有所改善,尤其是UC患者,其治疗效果与生物制剂天真的患者相似。未来的临床试验应仔细区分生物制剂失败与不耐受,以减少潜在的偏差。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


