Mengli Xiao, Kyle C Molina, Neil R Aggarwal, Laurel E Beaty, Tellen D Bennett, Nichole E Carlson, Lindsey E Fish, Mika K Hamer, Bethany M Kwan, David A Mayer, Jennifer L Peers, Matthew K Wynia, Adit A Ginde
{"title":"A Machine Learning Method for Allocating Scarce COVID-19 Monoclonal Antibodies.","authors":"Mengli Xiao, Kyle C Molina, Neil R Aggarwal, Laurel E Beaty, Tellen D Bennett, Nichole E Carlson, Lindsey E Fish, Mika K Hamer, Bethany M Kwan, David A Mayer, Jennifer L Peers, Matthew K Wynia, Adit A Ginde","doi":"10.1001/jamahealthforum.2024.2884","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>During the COVID-19 pandemic, the effective distribution of limited treatments became a crucial policy goal. Yet, limited research exists using electronic health record data and machine learning techniques, such as policy learning trees (PLTs), to optimize the distribution of scarce therapeutics.</p><p><strong>Objective: </strong>To evaluate whether a machine learning PLT-based method of scarce resource allocation optimizes the treatment benefit of COVID-19 neutralizing monoclonal antibodies (mAbs) during periods of resource constraint.</p><p><strong>Design, setting, and participants: </strong>This retrospective cohort study used electronic health record data from October 1, 2021, to December 11, 2021, for the training cohort and data from June 1, 2021, to October 1, 2021, for the testing cohort. The cohorts included patients who had positive test results for SARS-CoV-2 and qualified for COVID-19 mAb therapy based on the US Food and Drug Administration's emergency use authorization criteria, ascertained from the patient electronic health record. Only some of the qualifying candidates received treatment with mAbs. Data were analyzed between from January 2023 to May 2024.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was overall expected hospitalization, assessed as the potential reduction in overall expected hospitalization if the PLT-based allocation system was used. This was compared to observed allocation using risk differences.</p><p><strong>Results: </strong>Among 9542 eligible patients in the training cohort (5418 female [56.8%]; age distribution: 18-44 years, 4151 [43.5%]; 45-64 years, 3146 [33.0%]; and ≥65 years, 2245 [23.5%]), a total of 3862 (40.5%) received mAbs. Among 6248 eligible patients in the testing cohort (3416 female [54.7%]; age distribution: 18-44 years, 2827 [45.2%]; 45-64 years, 1927 [30.8%]; and ≥65 years, 1494 [23.9%]), a total of 1329 (21.3%) received mAbs. Treatment allocation using the trained PLT model led to an estimated 1.6% reduction (95% CI, -2.0% to -1.2%) in overall expected hospitalization compared to observed treatment allocation in the testing cohort. The visual assessment showed that the PLT-based point system had a larger reduction in 28-day hospitalization compared with the Monoclonal Antibody Screening Score (maximum overall hospitalization difference, -1.0% [95% CI, -1.3% to -0.7%]) in the testing cohort.</p><p><strong>Conclusions and relevance: </strong>This retrospective cohort study proposes and tests a PLT method, which can be linked to a electronic health record data platform to improve real-time allocation of scarce treatments. Use of this PLT-based allocation method would have likely resulted in fewer hospitalizations across a population than were observed in usual care, with greater expected reductions than a commonly used point system.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"5 9","pages":"e242884"},"PeriodicalIF":11.3000,"publicationDate":"2024-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11400220/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2024.2884","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: During the COVID-19 pandemic, the effective distribution of limited treatments became a crucial policy goal. Yet, limited research exists using electronic health record data and machine learning techniques, such as policy learning trees (PLTs), to optimize the distribution of scarce therapeutics.
Objective: To evaluate whether a machine learning PLT-based method of scarce resource allocation optimizes the treatment benefit of COVID-19 neutralizing monoclonal antibodies (mAbs) during periods of resource constraint.
Design, setting, and participants: This retrospective cohort study used electronic health record data from October 1, 2021, to December 11, 2021, for the training cohort and data from June 1, 2021, to October 1, 2021, for the testing cohort. The cohorts included patients who had positive test results for SARS-CoV-2 and qualified for COVID-19 mAb therapy based on the US Food and Drug Administration's emergency use authorization criteria, ascertained from the patient electronic health record. Only some of the qualifying candidates received treatment with mAbs. Data were analyzed between from January 2023 to May 2024.
Main outcomes and measures: The primary outcome was overall expected hospitalization, assessed as the potential reduction in overall expected hospitalization if the PLT-based allocation system was used. This was compared to observed allocation using risk differences.
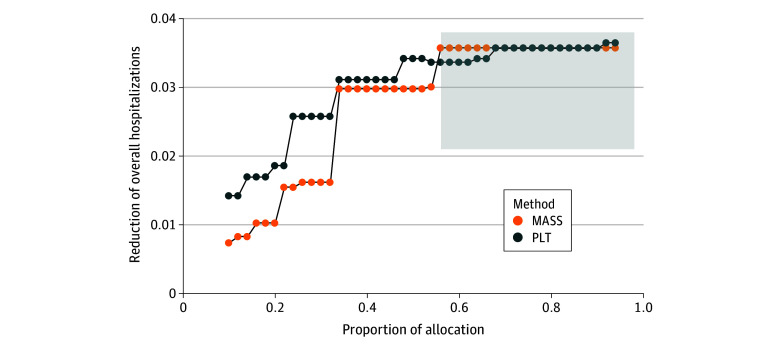
Results: Among 9542 eligible patients in the training cohort (5418 female [56.8%]; age distribution: 18-44 years, 4151 [43.5%]; 45-64 years, 3146 [33.0%]; and ≥65 years, 2245 [23.5%]), a total of 3862 (40.5%) received mAbs. Among 6248 eligible patients in the testing cohort (3416 female [54.7%]; age distribution: 18-44 years, 2827 [45.2%]; 45-64 years, 1927 [30.8%]; and ≥65 years, 1494 [23.9%]), a total of 1329 (21.3%) received mAbs. Treatment allocation using the trained PLT model led to an estimated 1.6% reduction (95% CI, -2.0% to -1.2%) in overall expected hospitalization compared to observed treatment allocation in the testing cohort. The visual assessment showed that the PLT-based point system had a larger reduction in 28-day hospitalization compared with the Monoclonal Antibody Screening Score (maximum overall hospitalization difference, -1.0% [95% CI, -1.3% to -0.7%]) in the testing cohort.
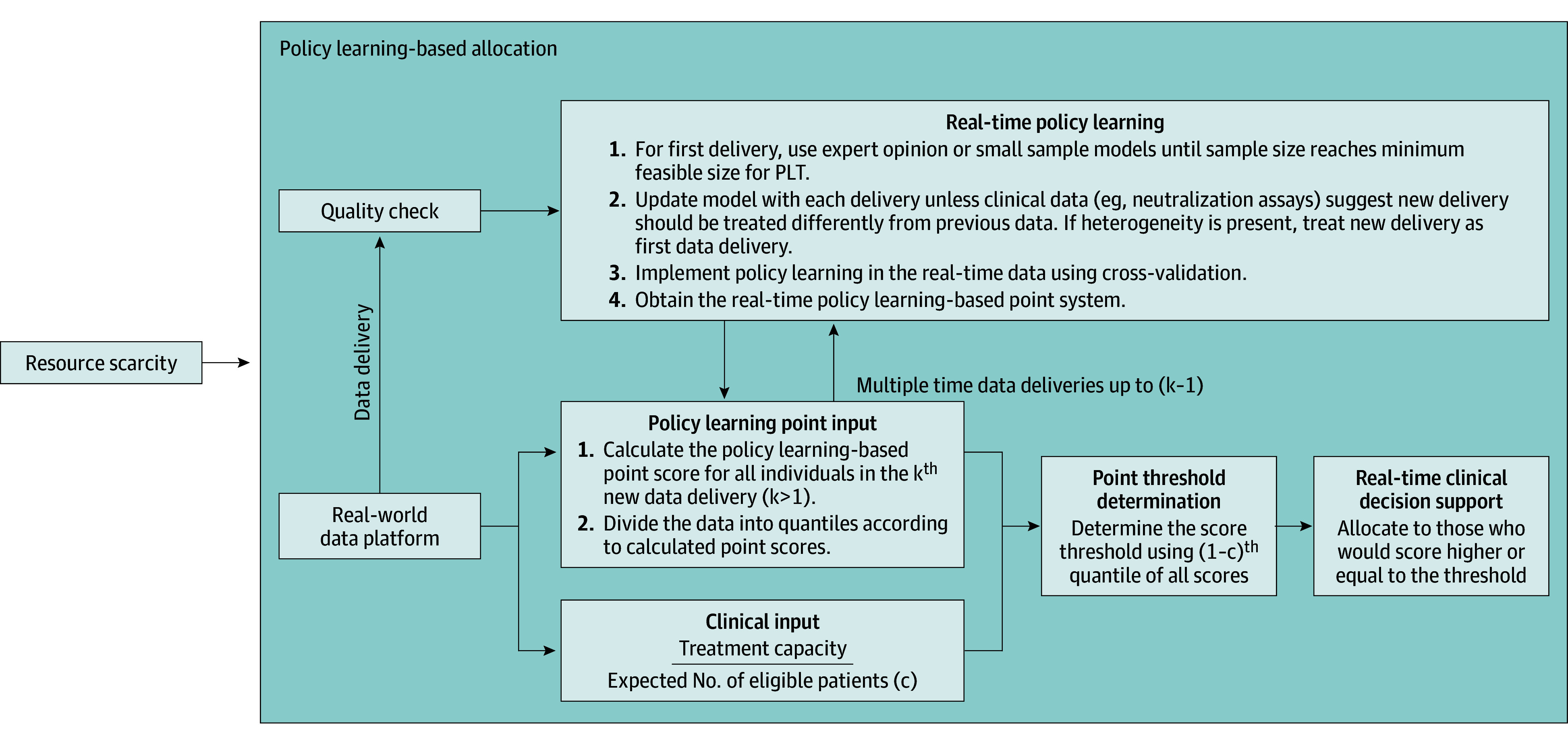
Conclusions and relevance: This retrospective cohort study proposes and tests a PLT method, which can be linked to a electronic health record data platform to improve real-time allocation of scarce treatments. Use of this PLT-based allocation method would have likely resulted in fewer hospitalizations across a population than were observed in usual care, with greater expected reductions than a commonly used point system.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


