Philipp Kriechling, Anna-Katharina Calek, Kimon Hatziisaak, Bettina Hochreiter, Samy Bouaicha, Karl Wieser
{"title":"Clinical Outcomes Do Not Deteriorate Over Time Following Primary Reverse Total Shoulder Arthroplasty: Minimum 10-Year Follow-up of 135 Shoulders.","authors":"Philipp Kriechling, Anna-Katharina Calek, Kimon Hatziisaak, Bettina Hochreiter, Samy Bouaicha, Karl Wieser","doi":"10.2106/JBJS.OA.23.00171","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Reverse total shoulder arthroplasty (RTSA) offers satisfactory mid-term outcomes for a variety of pathologies, but long-term follow-up data are limited. This study demonstrates the long-term clinical and radiographic outcomes as well as the predictive factors for an inferior outcome following RTSA.</p><p><strong>Methods: </strong>Using the prospective database of a single, tertiary referral center, we included all primary RTSAs that were performed during the study period and had a minimum 10-year follow-up. Clinical outcomes included the absolute Constant-Murley score (CS), relative CS, Subjective Shoulder Value (SSV), range of motion, pain, complication rate, and reintervention rate. Radiographic measurements included the critical shoulder angle (CSA), lateralization shoulder angle (LSA), distalization shoulder angle (DSA), reverse shoulder angle (RSA), acromiohumeral distance (ACHD), center of rotation, glenoid component height, notching, radiolucent lines, heterotopic ossification, and tuberosity resorption.</p><p><strong>Results: </strong>A total of 135 shoulders (133 patients) were available for analysis at a mean follow-up of 10.9 ± 1.6 years. The mean age was 69 ± 8 years, and 76 shoulders (76 patients; 56%) were female. For most of the clinical outcomes, initial improvements were observed in the short term and were sustained in the long term without notable deterioration, with >10-year follow-up values of 64 ± 16 for the absolute CS, 79% ± 18% for the relative CS, 79% ± 21% for the SSV, and 14 ± 3 for the CS for pain. However, after initial improvement, deterioration was seen for flexion and external rotation, with values of 117° ± 26° and 25° ± 18°, respectively, at the final follow-up. Scapular notching, heterotopic ossification, and radiolucent lines of <2 mm progressed during the study period. Younger age (p = 0.040), grade-II notching (p = 0.048), tuberosity resorption (p = 0.015), and radiolucent lines of <2 mm around the glenoid (p = 0.015) were predictive of an inferior outcome. The complication rate was 28%, with a reintervention rate of 11%.</p><p><strong>Conclusions: </strong>RTSA provided improved long-term results that did not significantly deteriorate over time for most of the clinical parameters. Negative clinical outcome predictors were younger age, grade-II notching, tuberosity resorption, and radiolucent lines of <2 mm around the glenoid.</p><p><strong>Level of evidence: </strong>Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"9 3","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11392479/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.23.00171","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Reverse total shoulder arthroplasty (RTSA) offers satisfactory mid-term outcomes for a variety of pathologies, but long-term follow-up data are limited. This study demonstrates the long-term clinical and radiographic outcomes as well as the predictive factors for an inferior outcome following RTSA.
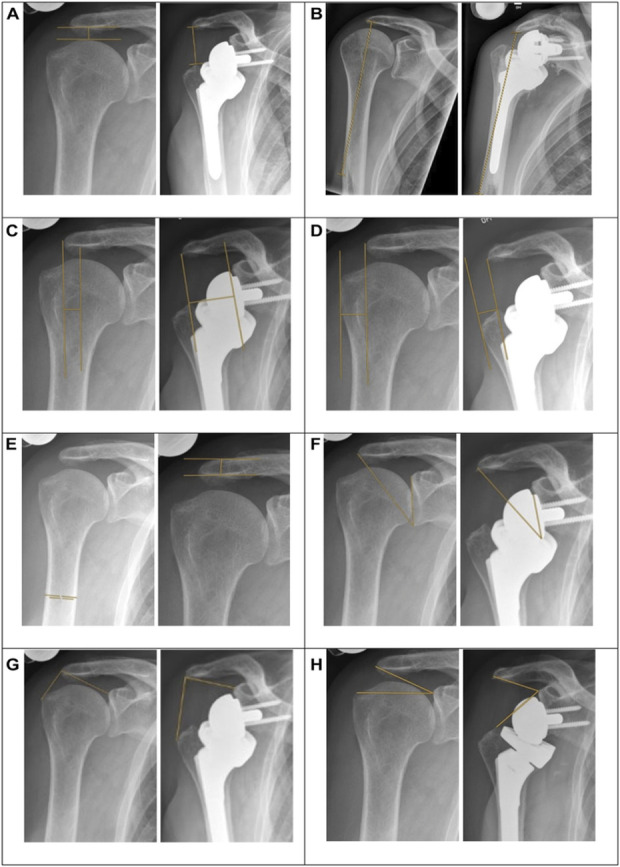
Methods: Using the prospective database of a single, tertiary referral center, we included all primary RTSAs that were performed during the study period and had a minimum 10-year follow-up. Clinical outcomes included the absolute Constant-Murley score (CS), relative CS, Subjective Shoulder Value (SSV), range of motion, pain, complication rate, and reintervention rate. Radiographic measurements included the critical shoulder angle (CSA), lateralization shoulder angle (LSA), distalization shoulder angle (DSA), reverse shoulder angle (RSA), acromiohumeral distance (ACHD), center of rotation, glenoid component height, notching, radiolucent lines, heterotopic ossification, and tuberosity resorption.
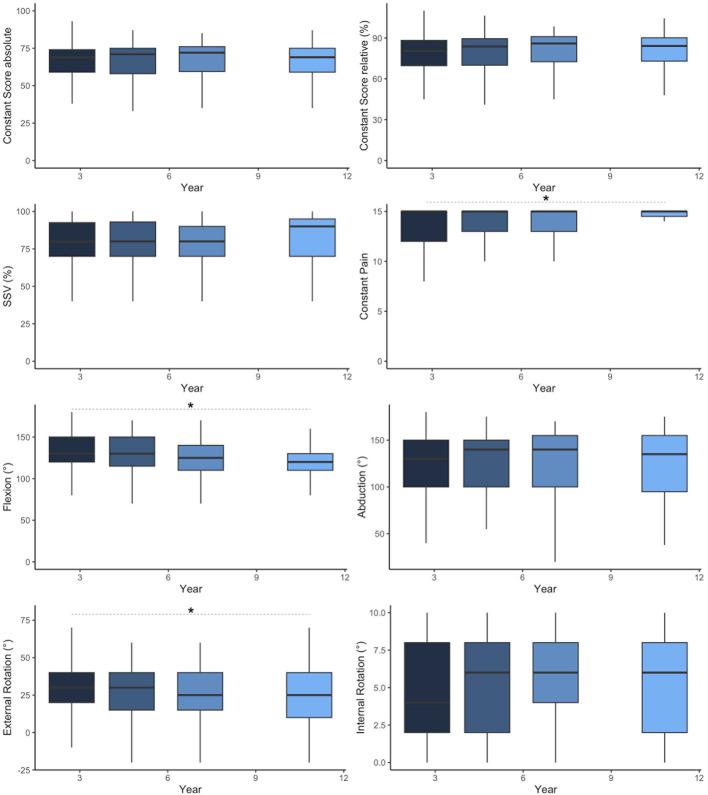
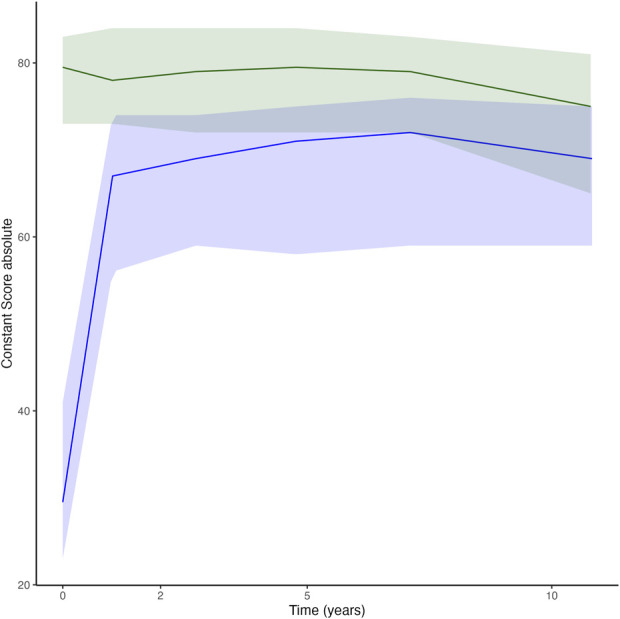
Results: A total of 135 shoulders (133 patients) were available for analysis at a mean follow-up of 10.9 ± 1.6 years. The mean age was 69 ± 8 years, and 76 shoulders (76 patients; 56%) were female. For most of the clinical outcomes, initial improvements were observed in the short term and were sustained in the long term without notable deterioration, with >10-year follow-up values of 64 ± 16 for the absolute CS, 79% ± 18% for the relative CS, 79% ± 21% for the SSV, and 14 ± 3 for the CS for pain. However, after initial improvement, deterioration was seen for flexion and external rotation, with values of 117° ± 26° and 25° ± 18°, respectively, at the final follow-up. Scapular notching, heterotopic ossification, and radiolucent lines of <2 mm progressed during the study period. Younger age (p = 0.040), grade-II notching (p = 0.048), tuberosity resorption (p = 0.015), and radiolucent lines of <2 mm around the glenoid (p = 0.015) were predictive of an inferior outcome. The complication rate was 28%, with a reintervention rate of 11%.
Conclusions: RTSA provided improved long-term results that did not significantly deteriorate over time for most of the clinical parameters. Negative clinical outcome predictors were younger age, grade-II notching, tuberosity resorption, and radiolucent lines of <2 mm around the glenoid.
Level of evidence: Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


