{"title":"Emergency Department and Critical Care Use of Clevidipine for Treatment of Hypertension in Patients With Acute Stroke.","authors":"Scott S Brehaut, Angelina M Roche","doi":"10.1097/HPC.0000000000000375","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Clevidipine is a parenteral dihydropyridine calcium channel blocker that received Food and Drug Administration approval in 2008 for the reduction of blood pressure (BP) when oral therapy is not feasible or not desirable. Soon after approval, our institution incorporated clevidipine into protocols for the management of hypertension among acute stroke patients, based on the drug's rapid onset of action and straightforward titration to goal. A subsequent retrospective review of its use in otherwise alteplase-eligible ischemic stroke patients with BP greater than 185/110 mm Hg (n = 32, in 2014) revealed that clevidipine in that setting demonstrated the shortest median time to BP control, the shortest median door-to-alteplase administration time, and the lowest administered volume of any parenteral antihypertensive used. As a result, clinical protocols in our institution were modified to make clevidipine first-line antihypertensive in both ischemic and hemorrhagic acute stroke. In this study, we report our institution's experience with clevidipine in acute stroke, comprising the largest such report to date.</p><p><strong>Methods: </strong>We conducted a retrospective chart review of all acute stroke patients who received clevidipine in the emergency department (ED) or intensive care unit (ICU) (n = 295) for the management of clinically significant hypertension between January 1, 2015, and December 31, 2017. Metrics analyzed included target (goal) BP for thrombolysis eligibility among patients intended for lytic therapy according to stroke management guidelines in effect at the time of care.</p><p><strong>Results: </strong>The median time for initial parenteral antihypertensive dose to goal (DTG) BP for all ischemic stroke patients (both those intended for and those not intended for lytic therapy) with complete data (n = 71 of 204) was 15 minutes; median time for door-to-IV-alteplase administration for ischemic stroke patients with complete data (n = 14 of 34 treated patients) was 59 minutes. The median time for initial parenteral antihypertensive DTG BP for all hemorrhagic stroke patients with complete data (n = 33 of 91 treated patients) was 39 minutes.</p><p><strong>Conclusions: </strong>We conclude that the salutary findings of the initial small study are valid across a larger patient sample of all acute stroke types. Based on these data, clevidipine is shown to be safe, consistent, and effective in the treatment of acute hypertension in ischemic and hemorrhagic stroke events, and is a reasonable first-line treatment option for acute hypertension in this setting.</p>","PeriodicalId":35914,"journal":{"name":"Critical Pathways in Cardiology","volume":" ","pages":"e0375"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11841717/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Pathways in Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/HPC.0000000000000375","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: Clevidipine is a parenteral dihydropyridine calcium channel blocker that received Food and Drug Administration approval in 2008 for the reduction of blood pressure (BP) when oral therapy is not feasible or not desirable. Soon after approval, our institution incorporated clevidipine into protocols for the management of hypertension among acute stroke patients, based on the drug's rapid onset of action and straightforward titration to goal. A subsequent retrospective review of its use in otherwise alteplase-eligible ischemic stroke patients with BP greater than 185/110 mm Hg (n = 32, in 2014) revealed that clevidipine in that setting demonstrated the shortest median time to BP control, the shortest median door-to-alteplase administration time, and the lowest administered volume of any parenteral antihypertensive used. As a result, clinical protocols in our institution were modified to make clevidipine first-line antihypertensive in both ischemic and hemorrhagic acute stroke. In this study, we report our institution's experience with clevidipine in acute stroke, comprising the largest such report to date.
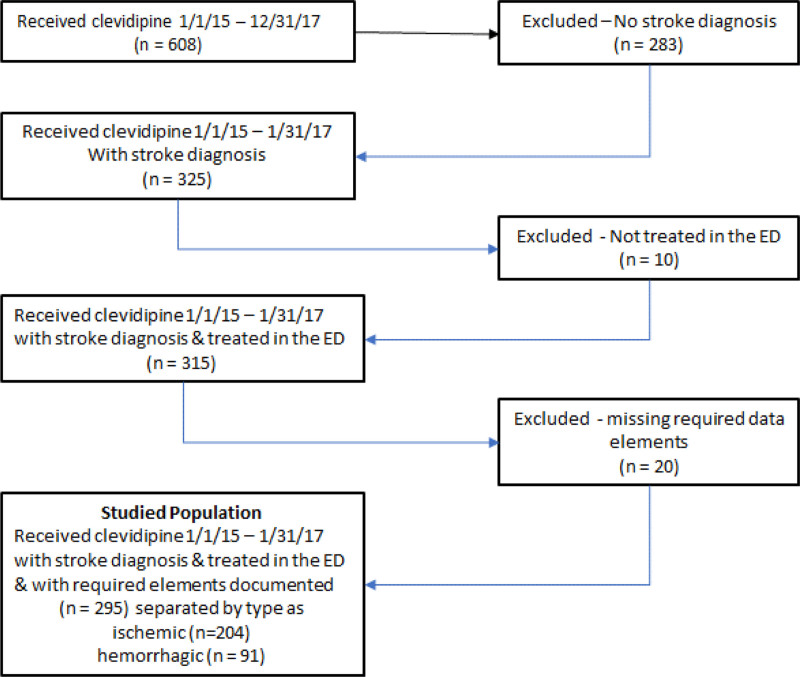
Methods: We conducted a retrospective chart review of all acute stroke patients who received clevidipine in the emergency department (ED) or intensive care unit (ICU) (n = 295) for the management of clinically significant hypertension between January 1, 2015, and December 31, 2017. Metrics analyzed included target (goal) BP for thrombolysis eligibility among patients intended for lytic therapy according to stroke management guidelines in effect at the time of care.
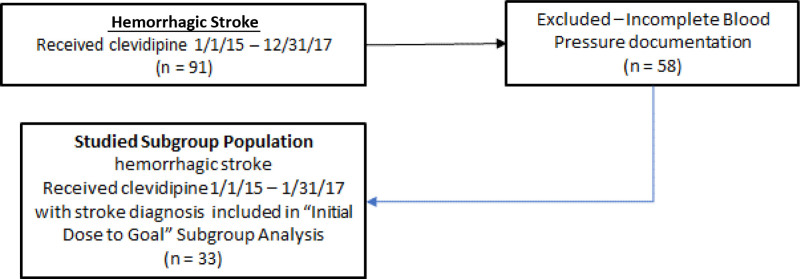
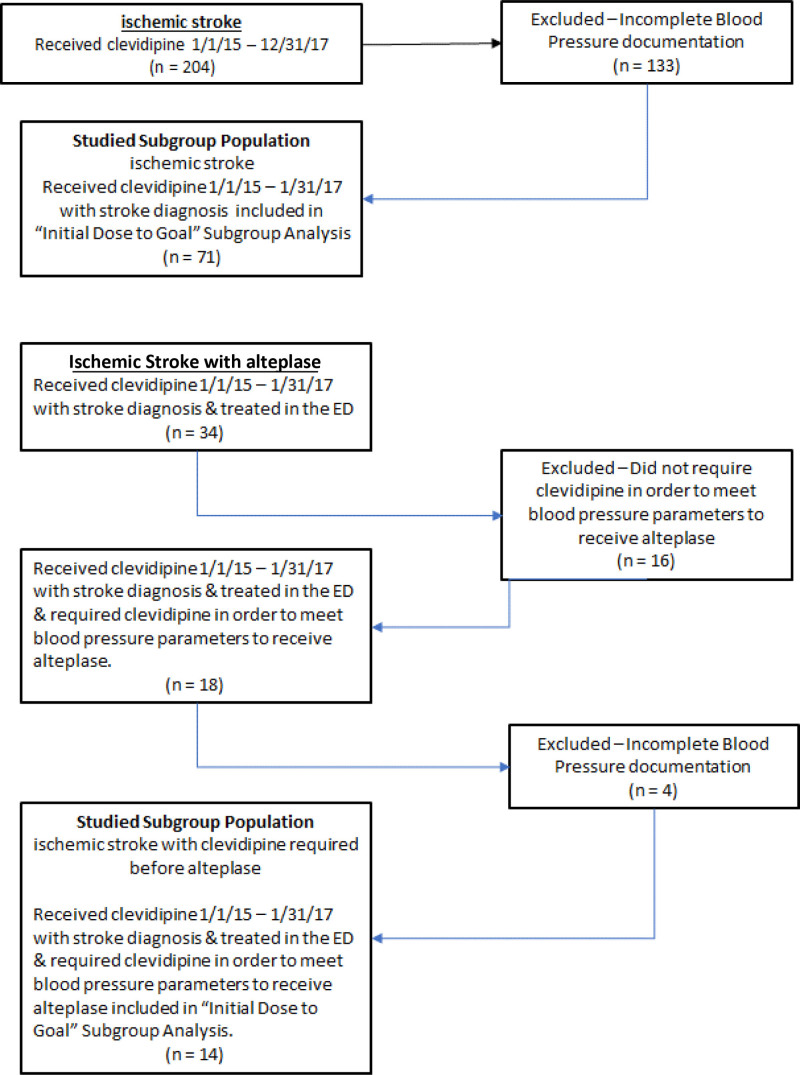
Results: The median time for initial parenteral antihypertensive dose to goal (DTG) BP for all ischemic stroke patients (both those intended for and those not intended for lytic therapy) with complete data (n = 71 of 204) was 15 minutes; median time for door-to-IV-alteplase administration for ischemic stroke patients with complete data (n = 14 of 34 treated patients) was 59 minutes. The median time for initial parenteral antihypertensive DTG BP for all hemorrhagic stroke patients with complete data (n = 33 of 91 treated patients) was 39 minutes.
Conclusions: We conclude that the salutary findings of the initial small study are valid across a larger patient sample of all acute stroke types. Based on these data, clevidipine is shown to be safe, consistent, and effective in the treatment of acute hypertension in ischemic and hemorrhagic stroke events, and is a reasonable first-line treatment option for acute hypertension in this setting.
期刊介绍:
Critical Pathways in Cardiology provides a single source for the diagnostic and therapeutic protocols in use at hospitals worldwide for patients with cardiac disorders. The Journal presents critical pathways for specific diagnoses—complete with evidence-based rationales—and also publishes studies of these protocols" effectiveness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


