Monica Sorbini, Enrico Aidala, Tullia Carradori, Francesco Edoardo Vallone, Gabriele Maria Togliatto, Cristiana Caorsi, Morteza Mansouri, Paola Burlo, Tiziana Vaisitti, Antonio Amoroso, Silvia Deaglio, Carlo Pace Napoleone
{"title":"Donor-derived Cell-free DNA Evaluation in Pediatric Heart Transplant Recipients: A Single-center 12-mo Experience.","authors":"Monica Sorbini, Enrico Aidala, Tullia Carradori, Francesco Edoardo Vallone, Gabriele Maria Togliatto, Cristiana Caorsi, Morteza Mansouri, Paola Burlo, Tiziana Vaisitti, Antonio Amoroso, Silvia Deaglio, Carlo Pace Napoleone","doi":"10.1097/TXD.0000000000001689","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endomyocardial biopsy (EMB) is considered the gold-standard method to diagnose rejection after heart transplantation. However, the many disadvantages and potential complications of this test restrict its routine application, particularly in pediatric patients. Donor-derived cell-free DNA (dd-cfDNA), released by the transplanted heart as result of cellular injury, is emerging as a biomarker of tissue damage involved in ischemia/reperfusion injury and posttransplant rejection. In the present study, we systematically evaluated dd-cfDNA levels in pediatric heart transplant patients coming for follow-up visits to our clinic for 12 mo, with the aim of determining whether dd-cfDNA monitoring could be efficiently applied and integrated into the posttransplant management of rejection in pediatric recipients.</p><p><strong>Methods: </strong>Twenty-nine patients were enrolled, and cfDNA was obtained from 158 blood samples collected during posttransplant follow-up. dd-cfDNA% was determined with a droplet-digital polymerase chain reaction assay. EMB scores, donor-specific antibody measurements, and distress marker quantification were correlated with dd-cfDNA, together with echocardiogram information.</p><p><strong>Results: </strong>The percentage of dd-cfDNA increased when EMBs scored positive for rejection (<i>P</i> = 0.0002) and donor-specific antibodies were present (<i>P</i> = 0.0010). N-terminal pro-B-type natriuretic peptide and high-sensitive troponin I elevation were significantly associated with dd-cfDNA release (<i>P</i> = 0.02 and <i>P</i> < 0.0001, respectively), as were reduced isovolumetric relaxation time (<i>P</i> = 0.0031), signs of heart failure (<i>P</i> = 0.0018), and treatment for rejection (<i>P</i> = 0.0017). By determining a positive threshold for rejection at 0.55%, the test had a negative predictive value maximized at 100%.</p><p><strong>Conclusions: </strong>Collectively, results indicate that dd-cfDNA monitoring has a high negative prognostic value, suggesting that in heart transplanted children with dd-cfDNA levels of <0.55% threshold, protocol EMBs may be postponed.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"10 10","pages":"e1689"},"PeriodicalIF":1.9000,"publicationDate":"2024-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11410329/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001689","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
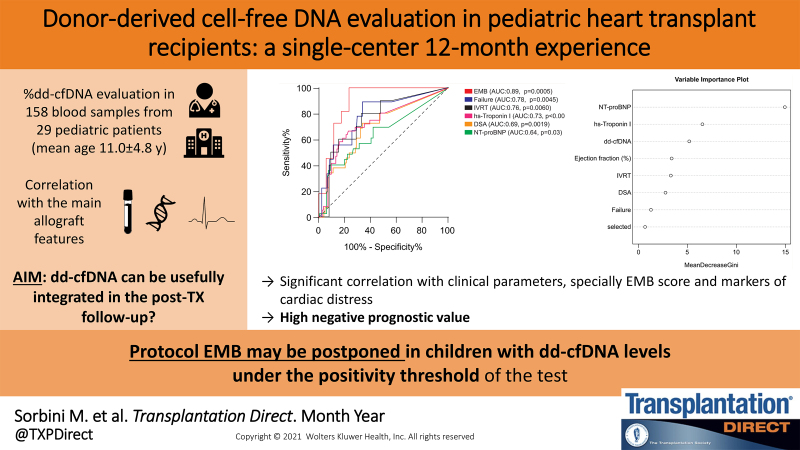
Background: Endomyocardial biopsy (EMB) is considered the gold-standard method to diagnose rejection after heart transplantation. However, the many disadvantages and potential complications of this test restrict its routine application, particularly in pediatric patients. Donor-derived cell-free DNA (dd-cfDNA), released by the transplanted heart as result of cellular injury, is emerging as a biomarker of tissue damage involved in ischemia/reperfusion injury and posttransplant rejection. In the present study, we systematically evaluated dd-cfDNA levels in pediatric heart transplant patients coming for follow-up visits to our clinic for 12 mo, with the aim of determining whether dd-cfDNA monitoring could be efficiently applied and integrated into the posttransplant management of rejection in pediatric recipients.
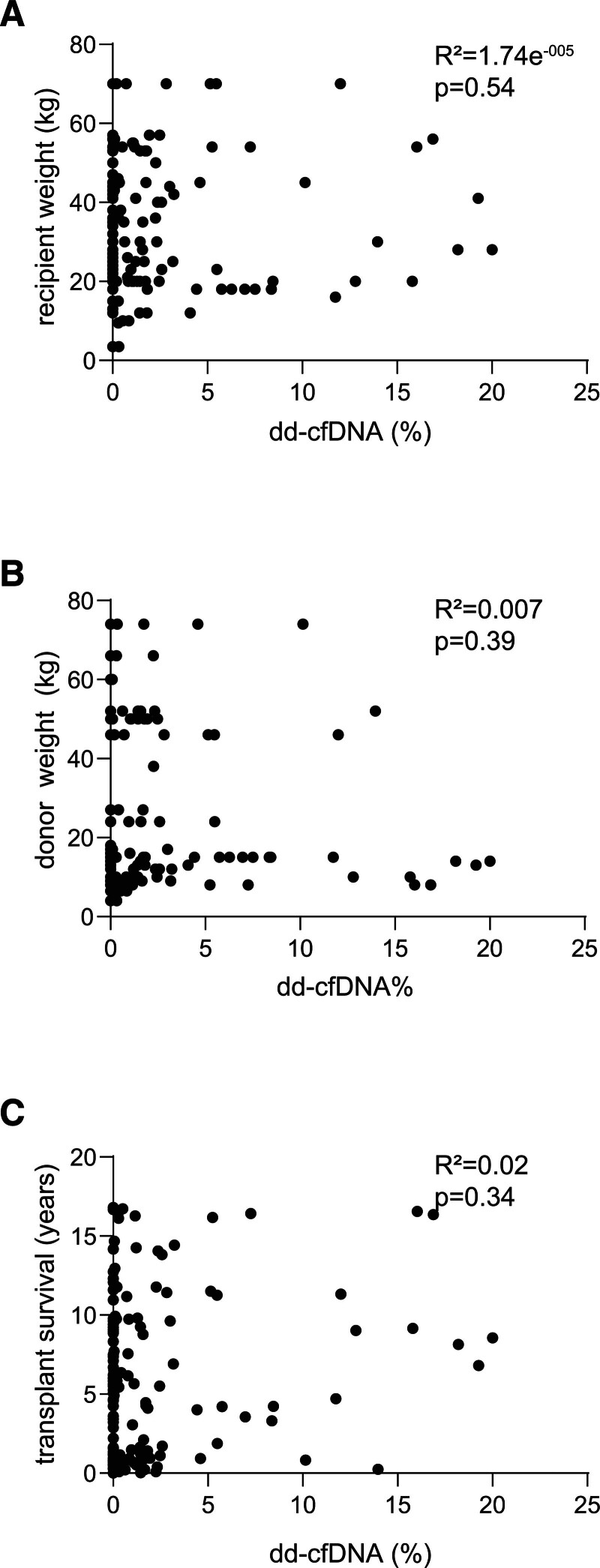
Methods: Twenty-nine patients were enrolled, and cfDNA was obtained from 158 blood samples collected during posttransplant follow-up. dd-cfDNA% was determined with a droplet-digital polymerase chain reaction assay. EMB scores, donor-specific antibody measurements, and distress marker quantification were correlated with dd-cfDNA, together with echocardiogram information.
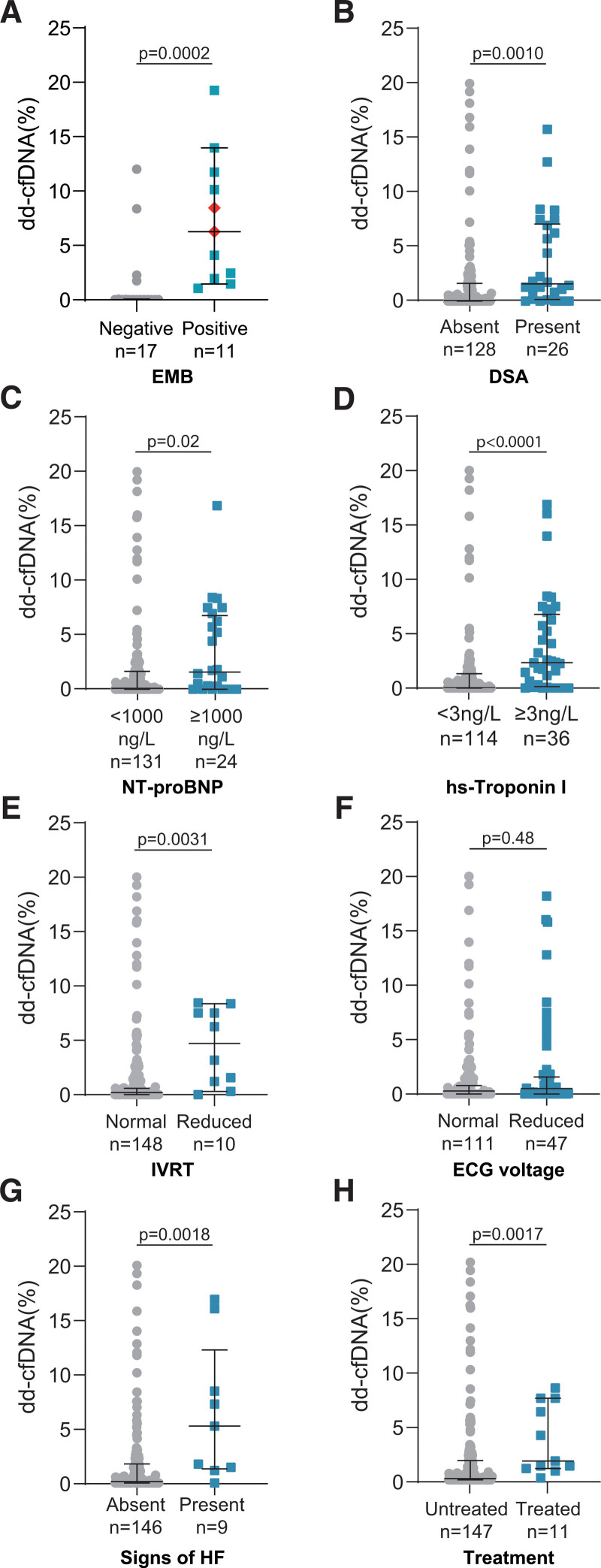
Results: The percentage of dd-cfDNA increased when EMBs scored positive for rejection (P = 0.0002) and donor-specific antibodies were present (P = 0.0010). N-terminal pro-B-type natriuretic peptide and high-sensitive troponin I elevation were significantly associated with dd-cfDNA release (P = 0.02 and P < 0.0001, respectively), as were reduced isovolumetric relaxation time (P = 0.0031), signs of heart failure (P = 0.0018), and treatment for rejection (P = 0.0017). By determining a positive threshold for rejection at 0.55%, the test had a negative predictive value maximized at 100%.
Conclusions: Collectively, results indicate that dd-cfDNA monitoring has a high negative prognostic value, suggesting that in heart transplanted children with dd-cfDNA levels of <0.55% threshold, protocol EMBs may be postponed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


