Effect of Preoperative Intravenous and Inhalational Dexmedetomidine on the Hemodynamic Response of Laryngoscopy: A Prospective Double-blinded Randomized Study.
{"title":"Effect of Preoperative Intravenous and Inhalational Dexmedetomidine on the Hemodynamic Response of Laryngoscopy: A Prospective Double-blinded Randomized Study.","authors":"Shivanya Singh, Priyanka Gupta, Mridul Dhar, Arhan Pasha","doi":"10.4103/jrpp.jrpp_12_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Laryngoscopy induces potent noxious stimuli causing reflex autonomic activation manifested by an increase in blood pressure and heart rate (HR). Various drugs with different routes have been tried to prevent this response. The literature comparing inhalational dexmedetomidine with intravenous (IV) dexmedetomidine to prevent laryngoscopy response is limited.</p><p><strong>Methods: </strong>A total of 150 American Society of Anesthesiologists Physical Status Class I/II, undergoing elective surgery requiring laryngoscopy and intubation, were included and randomized into two groups. Patients in Group D<sub>INH</sub> received nebulized dexmedetomidine (1 μg/kg) and in Group D<sub>IV</sub> received IV dexmedetomidine (0.5 μg/kg), 15 min before anesthesia induction. For blinding, nebulized or IV saline was used simultaneously. The primary outcome was to compare the mean arterial pressure (MAP) and HR at laryngoscopy, intubation, and 1, 5, and 10 min after intubation. The secondary outcome was to compare sedation, following the administration of dexmedetomidine, propofol consumption during induction, and any side effects.</p><p><strong>Findings: </strong>There was no significant difference in MAP (mmHg) postlaryngoscopy and intubation (immediate after intubation 78.5 ± 11.3 vs. 82.3 ± 16.0, <i>P</i> = 0.093). The mean HR was clinically similar in both groups postlaryngoscopy and intubation (immediate after intubation, 80.9 ± 12.5 vs. 76.3 ± 10.9). Patients in the D<sub>IV</sub> group were more sedated than the D<sub>INH</sub> (Ramsay Sedation Scale 3-4 vs. 1-2, <i>P</i> < 0.001). Bradycardia was seen in eight patients of the D<sub>IV</sub> group only.</p><p><strong>Conclusion: </strong>Preoperative nebulized dexmedetomidine is as effective as and safer than IV dexmedetomidine in preventing laryngoscopic response among adults.</p>","PeriodicalId":17158,"journal":{"name":"Journal of Research in Pharmacy Practice","volume":"12 4","pages":"123-129"},"PeriodicalIF":0.7000,"publicationDate":"2024-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11386063/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Research in Pharmacy Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jrpp.jrpp_12_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Laryngoscopy induces potent noxious stimuli causing reflex autonomic activation manifested by an increase in blood pressure and heart rate (HR). Various drugs with different routes have been tried to prevent this response. The literature comparing inhalational dexmedetomidine with intravenous (IV) dexmedetomidine to prevent laryngoscopy response is limited.
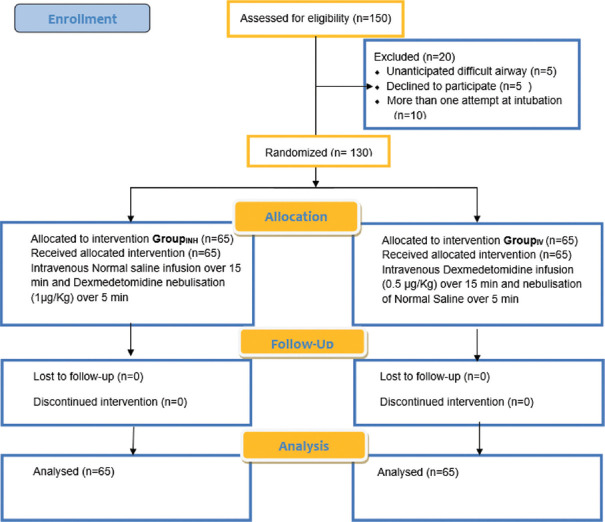
Methods: A total of 150 American Society of Anesthesiologists Physical Status Class I/II, undergoing elective surgery requiring laryngoscopy and intubation, were included and randomized into two groups. Patients in Group DINH received nebulized dexmedetomidine (1 μg/kg) and in Group DIV received IV dexmedetomidine (0.5 μg/kg), 15 min before anesthesia induction. For blinding, nebulized or IV saline was used simultaneously. The primary outcome was to compare the mean arterial pressure (MAP) and HR at laryngoscopy, intubation, and 1, 5, and 10 min after intubation. The secondary outcome was to compare sedation, following the administration of dexmedetomidine, propofol consumption during induction, and any side effects.
Findings: There was no significant difference in MAP (mmHg) postlaryngoscopy and intubation (immediate after intubation 78.5 ± 11.3 vs. 82.3 ± 16.0, P = 0.093). The mean HR was clinically similar in both groups postlaryngoscopy and intubation (immediate after intubation, 80.9 ± 12.5 vs. 76.3 ± 10.9). Patients in the DIV group were more sedated than the DINH (Ramsay Sedation Scale 3-4 vs. 1-2, P < 0.001). Bradycardia was seen in eight patients of the DIV group only.
Conclusion: Preoperative nebulized dexmedetomidine is as effective as and safer than IV dexmedetomidine in preventing laryngoscopic response among adults.
期刊介绍:
The main focus of the journal will be on evidence-based drug-related medical researches (with clinical pharmacists’ intervention or documentation), particularly in the Eastern Mediterranean region. However, a wide range of closely related issues will be also covered. These will include clinical studies in the field of pharmaceutical care, reporting adverse drug reactions and human medical toxicology, pharmaco-epidemiology and toxico-epidemiology (poisoning epidemiology), social aspects of pharmacy practice, pharmacy education and economic evaluations of treatment protocols (e.g. cost-effectiveness studies). Local reports of medication utilization studies at hospital or pharmacy levels will only be considered for peer-review process only if they have a new and useful message for the international pharmacy practice professionals and readers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


