Hertzel C. Gerstein MD, Mu Yang MSc, Shun Fu Lee PhD, Kelley R. H. Branch MD, Stefano Del Prato MD, Carolyn S. P. Lam MBBS, Renato D. Lopes MD, Richard Pratley MD, Julio Rosenstock MD, Naveed Sattar FmedSci
{"title":"Do nonglycaemic effects such as weight loss account for HbA1c lowering with efpeglenatide?: Insights from the AMPLITUDE-O trial","authors":"Hertzel C. Gerstein MD, Mu Yang MSc, Shun Fu Lee PhD, Kelley R. H. Branch MD, Stefano Del Prato MD, Carolyn S. P. Lam MBBS, Renato D. Lopes MD, Richard Pratley MD, Julio Rosenstock MD, Naveed Sattar FmedSci","doi":"10.1111/dom.15957","DOIUrl":null,"url":null,"abstract":"<p>Glucagon-like-peptide-1 receptor agonists (GLP-1 RA) lower HbA1c by promoting insulin secretion in response to elevated glucose (the incretin effect).<span><sup>1, 2</sup></span> They also slow gastric emptying; reduce appetite, weight, blood pressure, low-density lipoprotein (LDL) cholesterol and serious health outcomes<span><sup>3</sup></span>; and increase heart rate and pancreatic enzymes. The degree to which these nonglycaemic effects mediate their glycaemic effects remains unclear.</p><p>In the AMPLITUDE-O trial, people with type 2 diabetes mellitus (T2DM) and previous cardiovascular or kidney disease were randomly assigned to weekly injections of the GLP-1 RA efpeglenatide or placebo. During a median follow-up of 1.8 years, efpeglenatide reduced major adverse cardiovascular events by 27%.<span><sup>4</sup></span> It also reduced HbA1c by 1.24%, reaching a nadir within 3 months. Efpeglenatide's effect on other measurements during this period and the degree to which these changes statistically accounted for or mediated its effect on HbA1c are presented here.</p><p>The AMPLITUDE-O trial was conducted at 344 sites in 28 countries.<span><sup>4, 5</sup></span> It recruited people with T2DM and a HbA1c >7% with either prior cardiovascular disease or prior kidney disease, and randomly assigned them to weekly subcutaneous injections of placebo, efpeglenatide 4 mg weekly or efpeglenatide 6 mg. Continuous variables were measured at baseline, at 3 months and at various subsequent time points (depending on the variable).</p><p>The 4076 AMPLITUDE-O participants (33% women) were of mean age 64.5 ± 8.2 years with a mean duration of diabetes of 15.4 ± 8.8 years<span><sup>4</sup></span>; 90% had prior cardiovascular disease, 32% had prior kidney disease, 63% were taking insulin, 73% were taking metformin, 25% were taking a sulfonylurea and 15% were taking an SGLT2 inhibitor. Between 3442 (87%) and 3940 (97%) of the 4076 participants had both a baseline and a 3-month value for HbA1c and 18 continuous variables (Table S1).</p><p>Table 1 shows that efpeglenatide (4 or 6 mg weekly) significantly reduced HbA1c by 1.46% (95% confidence interval [CI]: 1.40, 1.53) during the first 3 months of follow up. During this same period, efpeglenatide significantly reduced mean weight, systolic blood pressure, pulse pressure, albumin-to-creatinine ratio, total cholesterol, LDL cholesterol, high-density lipoprotein (HDL) cholesterol, triglyceride, alkaline phosphatase, alanine transaminase and FIB-4 score, and significantly increased heart rate, amylase and lipase.</p><p>When efpeglenatide's effect on HbA1c was additionally adjusted for its effect on each of the 14 variables that were also significantly changed by efpeglenatide, there was only a modest attenuation of its effect on HbA1c (Table S2). Figure 1 illustrates those variables for which the 3-month change attenuated the effect of efpeglenatide on the 3-month change in HbA1c by at least 1%. Notably, the effect of efpeglenatide on HbA1c varied with the change in weight, triglyceride, HDL cholesterol, and FIB-4 score (<i>p</i> for all these interactions ≤0.02). There was no evidence of nonlinearity in the relationship between changes in the possible mediating variables in Table S2 and changes in HbA1c after accounting for multiple testing (lowest <i>p</i>-value = 0.035).</p><p>When all change variables with an attenuation ≥1% were included in a multi-variable linear regression model (plus any significant efpeglenatide interaction terms), the estimated 3-month difference in HbA1c was 1.29 (95% CI: 1.20, 1.38), representing an 11.7% attenuation from 1.46 (95% CI: 1.40, 1.53)% derived from the model without these variables.</p><p>These analyses show that the effect of the GLP-1 RA efpeglenatide on HbA1c cannot be statistically explained by its effect on 18 variables. They also show that less than 3% of its glycaemic effect can be statistically explained by the mean weight loss of 1.9 kg, and less than 6% of its effect on HbA1c can be explained by its effects on lipids, surrogates of hepatic fibrosis, pancreatic exocrine cells or clinical measures. Indeed, efpeglenatide's effects on all these factors together account for less than 12% of its HbA1c effect.</p><p>Little is known regarding the degree to which the nonglycaemic effects of GLP-1 RAs are correlated with or can statistically explain their glucose-lowering effects. Other than the incretin effect itself, the most likely mediator of the glycaemic effect of this class of drugs is weight loss, as these drugs are effective weight-reducing agents.<span><sup>8</sup></span> This is supported by modest correlations between HbA1c reduction and weight loss,<span><sup>9</sup></span> and by evidence that diet- and drug-mediated weight loss as well as metabolic surgery clearly lowers glucose levels and can even achieve diabetes remission in many people with T2DM.<span><sup>10-13</sup></span> Nevertheless, the modest degree to which efpeglenatide’ s effect on weight accounted for its effect on HbA1c in this analysis of the AMPLITUDE-O results suggests that efpeglenatide's glucose and weight-related effects mostly act independently. The remaining analyses support the conclusion that the glycaemic effect of this drug is independent of any other nonglycaemic effects. This effect of an exendin-based GLP-1 RA may or may not be true for other GLP-1 RAs or related drugs that are associated with modest weight loss. Moreover, greater weight loss with other incretin drugs such as tirzepatide may conceivably have a greater impact on HbA1c reduction. Other unmeasured effects of GLP-1 RA drugs, including changes in the composition of the diet, could also be mediating some of the benefits on HbA1c.</p><p>Strengths of these analyses include the fact that they are based on data from a large randomized trial, that data were available in greater than 87% of all participants, that they focused on the first 3 months of therapy (when the effect of efpeglenatide on HbA1c was greatest) and that participants were typical of those prescribed a GLP-1 RA. They are limited by the short (3-month) window of analysis and the small number of people with a short duration of diabetes (in whom diet and weight loss may be most effective).</p><p>These findings therefore support the conclusion that most of efpeglenatide's glycaemic effect is due to its incretin-related effects. Whether the same is true for GLP-1 RA-related therapies that yield substantially greater weight loss needs further investigation.</p><p>Hertzel C. Gerstein wrote the first draft of the paper. Mu Yang and Shun Fu Lee performed the statistical analyses. All the authors collected the data and critically revised the paper. Hertzel C. Gerstein is the guarantor of the study and made the final decision to submit and publish the manuscript of this work; therefore, he had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.</p><p>Hertzel C. Gerstein holds the McMaster-Sanofi Population Health Institute Chair in Diabetes Research and Care. He reports research grants from Eli Lilly, AstraZeneca, Novo Nordisk, Hanmi and Merck; continuing education grants from Eli Lilly, Abbott, Sanofi, Novo Nordisk and Boehringer Ingelheim; honoraria for speaking from AstraZeneca, Eli Lilly, Novo Nordisk, DKSH, Zuellig, Sanofi, Carbon Brand and Jiangsu Hanson; and consulting fees from Abbott, Bayer, Eli Lilly, Novo Nordisk, Pfizer, Sanofi, Kowa and Hanmi. Kelley R. H. Branch receives research grants from Bayer, Sanofi, Eli Lilly, Kestra and Medic One Foundation, and reports consulting fees from Bayer, Janssen, Amgen, Sana, Kestra and Hanmi. Stefano Del Prato reports consulting fees from Abbott, Amarin Corporation, Applied Therapeutics, AstraZeneca, Eli Lilly and Company, Eva Pharma, Menarini International, Novo Nordisk, Sanofi and Sun Pharmaceuticals; received grant support from AstraZeneca and Boehringer Ingelheim; and received speaker fees from Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, Laboratori Guidotti, Menarini International, MSD, Novartis Pharmaceuticals, Novo Nordisk and Sanofi. Carolyn S. P. Lam is supported by a Clinician Scientist Award from the National Medical Research Council of Singapore and has received research support from NovoNordisk and Roche Diagnostics. She has served as a consultant or on the advisory board/steering committee/executive committee for Alleviant Medical, Allysta Pharma, AnaCardio AB, Applied Therapeutics, AstraZeneca, Bayer, Biopeutics, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, CardioRenal, CPC Clinical Research, Eli Lilly, Hanmi, Impulse Dynamics, Intellia Therapeutics, Ionis Pharmaceutical, Janssen Research & Development LLC, Medscape/WebMD Global LLC, Merck, Novartis, Novo Nordisk, Prosciento Inc., Quidel Corporation, Radcliffe Group Ltd., Recardio Inc., ReCor Medical, Roche Diagnostics, Sanofi, Siemens Healthcare Diagnostics and Us2.ai; and serves as the co-founder and non-executive director of Us2.ai. Renato D. Lopes reports research grants from Amgen, Boehringer Ingelheim, Bristol Myers Squibb, GlaxoSmithKline, Medtronic, Novo Nordisk, Pfizer and Sanofi US Services Inc.; and consulting fees from Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo Company, GlaxoSmithKline, Medtronic, Merck, Novo Nordisk, Pfizer, Portola Pharmaceuticals and Sanofi US Services Inc. Richard Pratley reports speaker fees from Lilly and Novo Nordisk; consulting fees from Bayer AG, Bayer HealthCare Pharmaceuticals Inc., Endogenex Inc., Gasherbrum Bio Inc., Genprex, Getz Pharma, Intas Pharmaceuticals Inc., Lilly, Novo Nordisk, Pfizer and Sun Pharmaceutical Industries; and grants from Biomea Fusion, Carmot Therapeutics, Dompe, Endogenex Inc., Fractyl, Lilly, Novo Nordisk and Sanofi. Julio Rosenstock reports clinical research grants from Applied Therapeutics, Biomea Fusion, Corcept, Boehringer Ingelheim, Eli Lilly and Company, Hanmi, Merck, Novartis, Novo Nordisk, Oramed, Pfizer and Sanofi; served on scientific advisory boards; and received honorarium or consulting fees from Applied Therapeutics, Biomea Fusion, Boehringer Ingelheim, Corcept, Eli Lilly and Company, Hanmi, Novo Nordisk, Oramed, Sanofi, Scholar Rock, Structure Therapeutics, Terns Pharma and Zealand; and received honoraria for lectures from Boehringer Ingelheim, Eli Lilly and Company, Novo Nordisk and Sanofi. Naveed Sattar has consulted for and/or received speaker honoraria from Abbott Laboratories, AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Janssen, Menarini-Ricerche, Novartis, Novo Nordisk, Pfizer, Roche Diagnostics and Sanofi; and received grant support paid to his university from AstraZeneca, Boehringer Ingelheim, Novartis and Roche Diagnostics outside the submitted work.</p>","PeriodicalId":158,"journal":{"name":"Diabetes, Obesity & Metabolism","volume":"26 12","pages":"6080-6084"},"PeriodicalIF":5.7000,"publicationDate":"2024-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/dom.15957","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes, Obesity & Metabolism","FirstCategoryId":"3","ListUrlMain":"https://dom-pubs.onlinelibrary.wiley.com/doi/10.1111/dom.15957","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Glucagon-like-peptide-1 receptor agonists (GLP-1 RA) lower HbA1c by promoting insulin secretion in response to elevated glucose (the incretin effect).1, 2 They also slow gastric emptying; reduce appetite, weight, blood pressure, low-density lipoprotein (LDL) cholesterol and serious health outcomes3; and increase heart rate and pancreatic enzymes. The degree to which these nonglycaemic effects mediate their glycaemic effects remains unclear.
In the AMPLITUDE-O trial, people with type 2 diabetes mellitus (T2DM) and previous cardiovascular or kidney disease were randomly assigned to weekly injections of the GLP-1 RA efpeglenatide or placebo. During a median follow-up of 1.8 years, efpeglenatide reduced major adverse cardiovascular events by 27%.4 It also reduced HbA1c by 1.24%, reaching a nadir within 3 months. Efpeglenatide's effect on other measurements during this period and the degree to which these changes statistically accounted for or mediated its effect on HbA1c are presented here.
The AMPLITUDE-O trial was conducted at 344 sites in 28 countries.4, 5 It recruited people with T2DM and a HbA1c >7% with either prior cardiovascular disease or prior kidney disease, and randomly assigned them to weekly subcutaneous injections of placebo, efpeglenatide 4 mg weekly or efpeglenatide 6 mg. Continuous variables were measured at baseline, at 3 months and at various subsequent time points (depending on the variable).
The 4076 AMPLITUDE-O participants (33% women) were of mean age 64.5 ± 8.2 years with a mean duration of diabetes of 15.4 ± 8.8 years4; 90% had prior cardiovascular disease, 32% had prior kidney disease, 63% were taking insulin, 73% were taking metformin, 25% were taking a sulfonylurea and 15% were taking an SGLT2 inhibitor. Between 3442 (87%) and 3940 (97%) of the 4076 participants had both a baseline and a 3-month value for HbA1c and 18 continuous variables (Table S1).
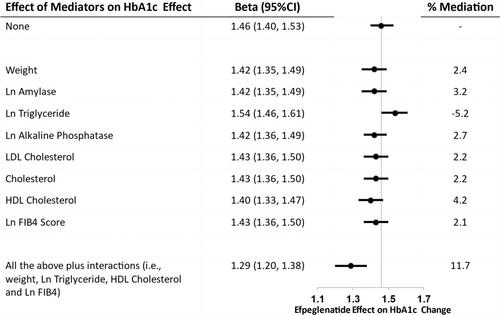
Table 1 shows that efpeglenatide (4 or 6 mg weekly) significantly reduced HbA1c by 1.46% (95% confidence interval [CI]: 1.40, 1.53) during the first 3 months of follow up. During this same period, efpeglenatide significantly reduced mean weight, systolic blood pressure, pulse pressure, albumin-to-creatinine ratio, total cholesterol, LDL cholesterol, high-density lipoprotein (HDL) cholesterol, triglyceride, alkaline phosphatase, alanine transaminase and FIB-4 score, and significantly increased heart rate, amylase and lipase.
When efpeglenatide's effect on HbA1c was additionally adjusted for its effect on each of the 14 variables that were also significantly changed by efpeglenatide, there was only a modest attenuation of its effect on HbA1c (Table S2). Figure 1 illustrates those variables for which the 3-month change attenuated the effect of efpeglenatide on the 3-month change in HbA1c by at least 1%. Notably, the effect of efpeglenatide on HbA1c varied with the change in weight, triglyceride, HDL cholesterol, and FIB-4 score (p for all these interactions ≤0.02). There was no evidence of nonlinearity in the relationship between changes in the possible mediating variables in Table S2 and changes in HbA1c after accounting for multiple testing (lowest p-value = 0.035).
When all change variables with an attenuation ≥1% were included in a multi-variable linear regression model (plus any significant efpeglenatide interaction terms), the estimated 3-month difference in HbA1c was 1.29 (95% CI: 1.20, 1.38), representing an 11.7% attenuation from 1.46 (95% CI: 1.40, 1.53)% derived from the model without these variables.
These analyses show that the effect of the GLP-1 RA efpeglenatide on HbA1c cannot be statistically explained by its effect on 18 variables. They also show that less than 3% of its glycaemic effect can be statistically explained by the mean weight loss of 1.9 kg, and less than 6% of its effect on HbA1c can be explained by its effects on lipids, surrogates of hepatic fibrosis, pancreatic exocrine cells or clinical measures. Indeed, efpeglenatide's effects on all these factors together account for less than 12% of its HbA1c effect.
Little is known regarding the degree to which the nonglycaemic effects of GLP-1 RAs are correlated with or can statistically explain their glucose-lowering effects. Other than the incretin effect itself, the most likely mediator of the glycaemic effect of this class of drugs is weight loss, as these drugs are effective weight-reducing agents.8 This is supported by modest correlations between HbA1c reduction and weight loss,9 and by evidence that diet- and drug-mediated weight loss as well as metabolic surgery clearly lowers glucose levels and can even achieve diabetes remission in many people with T2DM.10-13 Nevertheless, the modest degree to which efpeglenatide’ s effect on weight accounted for its effect on HbA1c in this analysis of the AMPLITUDE-O results suggests that efpeglenatide's glucose and weight-related effects mostly act independently. The remaining analyses support the conclusion that the glycaemic effect of this drug is independent of any other nonglycaemic effects. This effect of an exendin-based GLP-1 RA may or may not be true for other GLP-1 RAs or related drugs that are associated with modest weight loss. Moreover, greater weight loss with other incretin drugs such as tirzepatide may conceivably have a greater impact on HbA1c reduction. Other unmeasured effects of GLP-1 RA drugs, including changes in the composition of the diet, could also be mediating some of the benefits on HbA1c.
Strengths of these analyses include the fact that they are based on data from a large randomized trial, that data were available in greater than 87% of all participants, that they focused on the first 3 months of therapy (when the effect of efpeglenatide on HbA1c was greatest) and that participants were typical of those prescribed a GLP-1 RA. They are limited by the short (3-month) window of analysis and the small number of people with a short duration of diabetes (in whom diet and weight loss may be most effective).
These findings therefore support the conclusion that most of efpeglenatide's glycaemic effect is due to its incretin-related effects. Whether the same is true for GLP-1 RA-related therapies that yield substantially greater weight loss needs further investigation.
Hertzel C. Gerstein wrote the first draft of the paper. Mu Yang and Shun Fu Lee performed the statistical analyses. All the authors collected the data and critically revised the paper. Hertzel C. Gerstein is the guarantor of the study and made the final decision to submit and publish the manuscript of this work; therefore, he had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Hertzel C. Gerstein holds the McMaster-Sanofi Population Health Institute Chair in Diabetes Research and Care. He reports research grants from Eli Lilly, AstraZeneca, Novo Nordisk, Hanmi and Merck; continuing education grants from Eli Lilly, Abbott, Sanofi, Novo Nordisk and Boehringer Ingelheim; honoraria for speaking from AstraZeneca, Eli Lilly, Novo Nordisk, DKSH, Zuellig, Sanofi, Carbon Brand and Jiangsu Hanson; and consulting fees from Abbott, Bayer, Eli Lilly, Novo Nordisk, Pfizer, Sanofi, Kowa and Hanmi. Kelley R. H. Branch receives research grants from Bayer, Sanofi, Eli Lilly, Kestra and Medic One Foundation, and reports consulting fees from Bayer, Janssen, Amgen, Sana, Kestra and Hanmi. Stefano Del Prato reports consulting fees from Abbott, Amarin Corporation, Applied Therapeutics, AstraZeneca, Eli Lilly and Company, Eva Pharma, Menarini International, Novo Nordisk, Sanofi and Sun Pharmaceuticals; received grant support from AstraZeneca and Boehringer Ingelheim; and received speaker fees from Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, Laboratori Guidotti, Menarini International, MSD, Novartis Pharmaceuticals, Novo Nordisk and Sanofi. Carolyn S. P. Lam is supported by a Clinician Scientist Award from the National Medical Research Council of Singapore and has received research support from NovoNordisk and Roche Diagnostics. She has served as a consultant or on the advisory board/steering committee/executive committee for Alleviant Medical, Allysta Pharma, AnaCardio AB, Applied Therapeutics, AstraZeneca, Bayer, Biopeutics, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, CardioRenal, CPC Clinical Research, Eli Lilly, Hanmi, Impulse Dynamics, Intellia Therapeutics, Ionis Pharmaceutical, Janssen Research & Development LLC, Medscape/WebMD Global LLC, Merck, Novartis, Novo Nordisk, Prosciento Inc., Quidel Corporation, Radcliffe Group Ltd., Recardio Inc., ReCor Medical, Roche Diagnostics, Sanofi, Siemens Healthcare Diagnostics and Us2.ai; and serves as the co-founder and non-executive director of Us2.ai. Renato D. Lopes reports research grants from Amgen, Boehringer Ingelheim, Bristol Myers Squibb, GlaxoSmithKline, Medtronic, Novo Nordisk, Pfizer and Sanofi US Services Inc.; and consulting fees from Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo Company, GlaxoSmithKline, Medtronic, Merck, Novo Nordisk, Pfizer, Portola Pharmaceuticals and Sanofi US Services Inc. Richard Pratley reports speaker fees from Lilly and Novo Nordisk; consulting fees from Bayer AG, Bayer HealthCare Pharmaceuticals Inc., Endogenex Inc., Gasherbrum Bio Inc., Genprex, Getz Pharma, Intas Pharmaceuticals Inc., Lilly, Novo Nordisk, Pfizer and Sun Pharmaceutical Industries; and grants from Biomea Fusion, Carmot Therapeutics, Dompe, Endogenex Inc., Fractyl, Lilly, Novo Nordisk and Sanofi. Julio Rosenstock reports clinical research grants from Applied Therapeutics, Biomea Fusion, Corcept, Boehringer Ingelheim, Eli Lilly and Company, Hanmi, Merck, Novartis, Novo Nordisk, Oramed, Pfizer and Sanofi; served on scientific advisory boards; and received honorarium or consulting fees from Applied Therapeutics, Biomea Fusion, Boehringer Ingelheim, Corcept, Eli Lilly and Company, Hanmi, Novo Nordisk, Oramed, Sanofi, Scholar Rock, Structure Therapeutics, Terns Pharma and Zealand; and received honoraria for lectures from Boehringer Ingelheim, Eli Lilly and Company, Novo Nordisk and Sanofi. Naveed Sattar has consulted for and/or received speaker honoraria from Abbott Laboratories, AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Janssen, Menarini-Ricerche, Novartis, Novo Nordisk, Pfizer, Roche Diagnostics and Sanofi; and received grant support paid to his university from AstraZeneca, Boehringer Ingelheim, Novartis and Roche Diagnostics outside the submitted work.
期刊介绍:
Diabetes, Obesity and Metabolism is primarily a journal of clinical and experimental pharmacology and therapeutics covering the interrelated areas of diabetes, obesity and metabolism. The journal prioritises high-quality original research that reports on the effects of new or existing therapies, including dietary, exercise and lifestyle (non-pharmacological) interventions, in any aspect of metabolic and endocrine disease, either in humans or animal and cellular systems. ‘Metabolism’ may relate to lipids, bone and drug metabolism, or broader aspects of endocrine dysfunction. Preclinical pharmacology, pharmacokinetic studies, meta-analyses and those addressing drug safety and tolerability are also highly suitable for publication in this journal. Original research may be published as a main paper or as a research letter.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


