{"title":"Images of venipuncture injuries","authors":"Li Jiazhao PhD, Jiang Wenxin MD, Shen Yelin","doi":"10.1002/emp2.13278","DOIUrl":null,"url":null,"abstract":"<p>A 57-year-old female was admitted to the intensive care unit (ICU) following brain surgery. The process of deep venipuncture was challenging, as indicated by her lung computed tomography (CT) scans (Figures 1-3). Previously, she had a catheter in her left internal jugular vein, which was not functioning properly and was subsequently removed, leaving a retrosternal air leak shadow, as indicated by the red arrow in Figure 1. An attempt to puncture the right subclavian vein failed, resulting in residual gas trapped between the muscle layers (Figure 2) with a radius of 2 mm and an area of 13.21 mm<sup>2</sup>. Eventually, catheterization of the right internal jugular vein was successful after two failed attempts (Figure 3); some gas was observed near the catheter, with a maximum area of approximately 32 mm × 10 mm.</p><p>The patient's vital signs remained stable during and after the procedure. A follow-up lung CT performed 4 days later showed that all gas had been absorbed. However, deep venipuncture failures are common in clinical settings and can lead to complications,<span><sup>1</sup></span> such as mediastinal emphysema, peripheral nerve injury,<span><sup>2</sup></span> and pneumothorax, which in turn can result in economic burdens, prolonged hospitalization, and even fatalities—fortunately, this patient did not experience significant complications. However, the CT scan revealed past injuries, serving as a reminder for clinicians to exercise caution and rigor during invasive procedures.</p><p>The authors declare no conflict of interest.</p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 5","pages":""},"PeriodicalIF":1.6000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13278","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13278","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
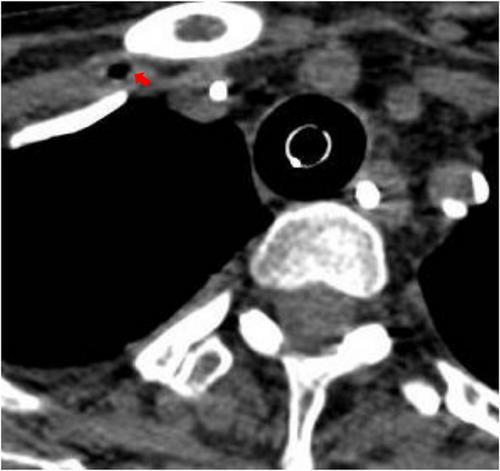
A 57-year-old female was admitted to the intensive care unit (ICU) following brain surgery. The process of deep venipuncture was challenging, as indicated by her lung computed tomography (CT) scans (Figures 1-3). Previously, she had a catheter in her left internal jugular vein, which was not functioning properly and was subsequently removed, leaving a retrosternal air leak shadow, as indicated by the red arrow in Figure 1. An attempt to puncture the right subclavian vein failed, resulting in residual gas trapped between the muscle layers (Figure 2) with a radius of 2 mm and an area of 13.21 mm2. Eventually, catheterization of the right internal jugular vein was successful after two failed attempts (Figure 3); some gas was observed near the catheter, with a maximum area of approximately 32 mm × 10 mm.
The patient's vital signs remained stable during and after the procedure. A follow-up lung CT performed 4 days later showed that all gas had been absorbed. However, deep venipuncture failures are common in clinical settings and can lead to complications,1 such as mediastinal emphysema, peripheral nerve injury,2 and pneumothorax, which in turn can result in economic burdens, prolonged hospitalization, and even fatalities—fortunately, this patient did not experience significant complications. However, the CT scan revealed past injuries, serving as a reminder for clinicians to exercise caution and rigor during invasive procedures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


