Does Wastewater Analysis Play a Role in Tracking Colorectal Cancer Hot Spots to Guide Geotargeted Neighborhood Interventions?
引用次数: 0
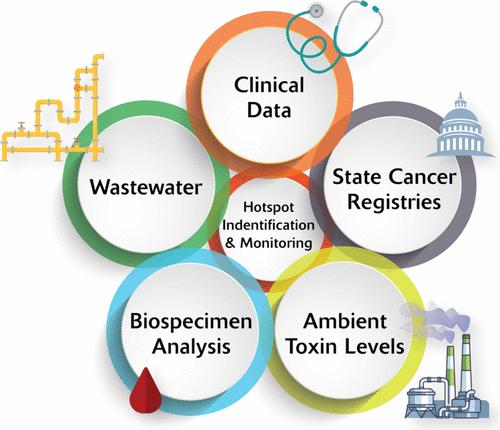
Abstract
Wastewater has been used as an early warning system to detect infectious disease outbreaks. (1,2) Extending this platform to monitor and survey areas with increased environmental health risks, such as volatile organic compound metabolites, (3) remains an unexplored opportunity. Globally, colorectal cancer (CRC) is ranked third for most common incidence and second for cancer-related mortality. (4,5) Despite a decline in CRC incidence rates among individuals who are ≥65 years of age (attributed largely to screening efforts), cases of early onset CRC (patients who are <50 years of age) are rapidly increasing, with the projected incidence rate doubling by 2030. (6) Talibov et al. (7) showed that exposure to volatile organic compounds in occupational settings was positively associated with CRC. Many high-risk populations that may be exposed to these compounds remain unscreened due healthcare disparities or due to age-related guidelines, (8) yet wastewater catches all ages. We advocate for further research aimed at integrating population-level environmental toxin wastewater data with existing patient and environmental health data sets to identify and track CRC hot spots and guide community-based interventions to decrease the incidence of CRC (Figure 1). Figure 1. Framework to enable better tracking of colorectal cancer hot spots with paired wastewater surveillance, ambient air monitoring, known registries, and biospecimens. Wastewater-based epidemiology provides an established approach for surveilling various population-sized areas, and its role in cancer hot spot tracking might be best at the neighborhood scale. A disproportionate number of patients with CRC residing in specific geographic areas may present to their local medical centers. Epidemiologists can monitor the CRC incidence rates using state cancer databases and integrate these rates with reports on ambient levels of environmental toxins. Biospecimens from patients with CRC residing within these identified areas can be triangulated with anonymous community-level wastewater samples for environmental pollutants that are geographically bound to neighborhood hot spots. Despite the overall increase in CRC screening rates, disparities persist in low-income communities and racially marginalized populations. (8) These populations experience higher levels of exposure to known environmental pollutants and barriers to access preventive and interventional healthcare services. A wastewater-based approach may allow for an increased intensity of community-level surveilling of populations at risk of CRC, including directed patient evaluations and CRC screening. This is analogous to SARS-CoV-2 infection testing, in which SARS-CoV-2 personal testing was inequitable and wastewater evaluation for SARS-CoV-2 enabled more equitable screening at a population level that informed neighborhood trends, even before COVID-19 symptoms became noticeable. Environmental surveillance data from wastewater may also provide insights into the lifetime environmental burdens that increase the risk of CRC. Wastewater evaluation of environmental carcinogens provides an additional avenue for cancer prevention. Residential proximity to industrial pollution sources has been attributed to CRC risk, presenting danger for the entire surrounding population instead of the historically described industrial workers. (9) Wastewater sampling allows the collection of data from defined geographic zones within communities, regardless of whether residents have pursued cancer screening or treatment or whether the onset is early or late, to promote CRC screening in such areas. By surveilling environmental carcinogens, as opposed to burdening the individual to overcome the structural barriers to CRC screening, public health departments can monitor and limit sources of environmental carcinogens, particularly in the neighborhoods that are known CRC hot spots. Wastewater may be a novel solution to CRC disparities with associated environmental injustices. Utilizing wastewater as an additional data source for CRC monitoring may not warrant the precision of lead time that was urgently needed during the COVID-19 pandemic. (1) It is unlikely that such an amount of data is needed for CRC monitoring; a yearly environmental toxin sample to guide geographic boundaries for community-based intervention may be most appropriate. Anderson et al. (10) reported neighborhood-level increased SARS-CoV-2 wastewater concentrations, leading to the successful implementation of a geotargeted advertising intervention to boost COVID-19 vaccination rates in high-risk neighborhoods. A complementary approach for CRC could be adopted to screen environmental toxins in wastewater and, when paired with ambient air monitoring, known registries, and biospecimens, alert geotargeted residents to their increased risk of developing CRC. With the added value of quantitative wastewater data, physicians can further enhance awareness by developing localized and culturally appropriate prevention strategies or by bolstering screening efforts. Collaborating with local organizations, cancer advocacy organizations can prioritize limited resources for planning and executing relevant and impactful yearly interventions in community zones rather than a uniform citywide intervention. Grassroots organizations can further advocate for their residents’ day-to-day health by backing initiatives for stricter control of industrial emissions and environmental cleanup efforts. Budget meetings also provide a platform for highlighting the importance of access to green spaces, nutritious foods, and affordable CRC screening, which work together to decrease the CRC burden on communities. Wastewater surveillance has the potential to be used in other public health areas, including cancer, particularly in urban areas with piped sewer networks. Wastewater may play a novel role in overcoming CRC racial and income disparities and the use of hot spot data to promote screening in neighborhoods that have less access to healthcare and include historically marginalized populations. CRC presents a significant public health challenge in the United States, particularly in early onset patients who are <50 years of age. The additive value of wastewater analysis provides a strong benefit for transdisciplinary integration by epidemiologists, physicians, environmental scientists, public health practitioners, and geographic researchers to stop, or at least slow, the increase in the number of CRC hot spots. T.S., N.D., and S.K. are joint senior authors. A.J. and R.H.H. drafted the article. All authors were involved in manuscript editing and were responsible for the decision to submit for publication. The University of Louisville Institutional Review Board approved this research as Human Subjects Research (IRB 23.0319). There is no patient/participant information included in this work, and thus, no applicable written informed consent was warranted. Rochelle H. Holm is an associate professor with the Christina Lee Brown Envirome Institute at the University of Louisville. Her current research includes surveillance of pathogen and environmental toxins across sewered and nonsewered sanitation systems. This work was supported by the Owsley Brown II Family Foundation, the NIH NIEHS University of Louisville (UofL) Center for Integrative Environmental Health Sciences (CIEHS) (P30 ES030283, N.D.), and UofL NIEHS Superfund Grant P42 ES023716 (N.D.). This article references 10 other publications. This article has not yet been cited by other publications.
废水分析在跟踪结直肠癌热点以指导有地理针对性的邻里干预中是否发挥作用?
有了定量废水数据的附加值,医生可以通过制定适合当地文化的预防策略或加强筛查工作,进一步提高人们的认识。癌症宣传机构可以与地方组织合作,将有限的资源优先用于规划和执行社区区域内相关且有影响力的年度干预措施,而不是全市统一的干预措施。基层组织可以通过支持更严格控制工业排放和环境清理工作的倡议,进一步倡导居民的日常健康。预算会议还提供了一个平台,可以强调获得绿地、营养食品和负担得起的 CRC 筛查的重要性,这些因素共同作用,可以减轻社区的 CRC 负担。废水监测有可能用于包括癌症在内的其他公共卫生领域,尤其是在拥有管道污水网络的城市地区。废水可在消除儿童癌变的种族和收入差距方面发挥新的作用,并可利用热点数据在较少获得医疗保健服务的社区以及历史上被边缘化的人群中推广筛查。在美国,CRC 是一项重大的公共卫生挑战,尤其是 50 岁以下的早发性患者。废水分析的附加值为流行病学家、医生、环境科学家、公共卫生从业人员和地理研究人员的跨学科整合提供了强大的益处,以阻止或至少减缓 CRC 热点数量的增加。T.S.、N.D.和S.K.为共同资深作者。A.J.和R.H.H.起草了文章。所有作者都参与了稿件编辑,并对是否投稿负责。路易斯维尔大学机构审查委员会批准本研究为人类受试者研究(IRB 23.0319)。本研究未包含患者/参与者信息,因此无需书面知情同意。Rochelle H. Holm 是路易斯维尔大学克里斯蒂娜-李-布朗环境研究所的副教授。她目前的研究包括监测下水道和非下水道卫生系统中的病原体和环境毒素。这项工作得到了欧斯利-布朗二世家族基金会、美国国立卫生研究院NIEHS路易斯维尔大学(UofL)综合环境健康科学中心(CIEHS)(P30 ES030283,N.D.)和路易斯维尔大学NIEHS超级基金拨款P42 ES023716(N.D.)的支持。本文引用了 10 篇其他出版物。本文尚未被其他出版物引用。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


