{"title":"Low methylthioadenosine phosphorylase expression is associated with worse survival in patients with acute myeloid leukaemia","authors":"Yiyu Xiao, Qianqian Peng, Advaith Maya Sanjeev Kumar, Houda Alachkar","doi":"10.1002/ctm2.70015","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor,</p><p>Deletions of methylthioadenosine phosphorylase (<i>MTAP</i>) are frequent in several malignancies and lead to 5′-deoxy-5′-methylthioadenosine (MTA) accumulation, competing with S-adenosylmethionine (SAM) for binding to Protein Arginine Methyltransferase 5 (PRMT5) and enhancing tumour sensitivity to PRMT5 inhibitors.<span><sup>1, 2</sup></span> Although MTAP enzyme deficiency has been documented in acute myeloid leukaemia (AML), deletions of the MTAP gene have not been identified in this haematological malignancy. Here we evaluated MTAP downregulation in AML datasets (TCGA and OHSU)<span><sup>3-7</sup></span> and its associations with clinical and molecular characteristics and patient's clinical outcome.</p><p>When comparing the <i>MTAP</i> expression between AML bone marrow (BM) (<i>n</i> = 542) and healthy BM (<i>n</i> = 73), different <i>MTAP</i> probes showed different results (MILE dataset,<span><sup>8</sup></span> Figure 1A–F). However, when comparing the GTEx and TCGA datasets on UCSC Xena,<span><sup>9</sup></span> we found higher <i>MTAP</i> expression in AML blood (<i>n</i> = 173) than normal blood samples (<i>n</i> = 337) (median-log2: 4.040 vs. −0.199, <i>p </i>= 6.596e<sup>−197</sup>, Figure 1G). Thirteen transcripts of MTAP were differentially expressed (Figure 1H). While only one deep deletion case was identified in AML in the TCGA dataset, using Z-score < −1 to define low expressor <i>MTAP</i>, we found 10.40% and 16.84% of cases have low <i>MTAP</i> expression in the TCGA and OHSU, respectively (Figure 1I).</p><p>To investigate whether low expression of <i>MTAP</i> is associated with specific baseline clinical features in patients with AML, we compared the frequency of <i>MTAP</i> low expression according to diagnosis age, sex, BM blast percentage, white blood cell count, peripheral blasts percentage, cytogenetic risk and molecular risk (Tables S1 and S2). In the TCGA dataset, we found <i>MTAP</i> low expression to be more frequent in older patients (diagnosis age ≥ 65 years) than in younger patients (diagnosis age < 65 years) (18.87% vs. 6.67%, <i>p </i>= .027). <i>MTAP</i> expression levels were found to be lower in patients with AML M3 (<i>n</i> = 16) than AML M2 (<i>n</i> = 38) (<i>p</i> = .030, Figure 2A).</p><p>We also assessed the association between <i>MTAP</i> low expression and AML molecular characteristics in terms of the presence of certain AML mutations (Tables S3 and S4). We compared the frequencies of <i>FLT3</i>, <i>DNMT3A</i>, <i>NPM1</i>, <i>IDH2</i>, <i>IDH1</i> and <i>TP53</i> mutations between low and unaltered/high <i>MTAP</i> patients. In OHSU, patients with MTAP low expression have a lower frequency of FLT3 mutations (17.3% vs. 32.1%, <i>p</i> = .036) and NPM1 mutation (3.8% vs. 30.6%, <i>p</i> < .001) compared with unaltered/high MTAP group. <i>MTAP</i> was expressed at significantly higher levels in patients with <i>NPM1</i> mutation (median-log2, TCGA: 1037 vs. 857.5, <i>p </i>= .0018, adjusted-<i>p</i> = .0112; OHSU: 4.058 vs. 3.606, <i>p </i>< .001, adjusted-<i>p</i> < .001), <i>DNMT3A</i> mutation (median-log2, TCGA: 980.3 vs. 844.0, <i>p</i> = .0094, adjusted-<i>p</i> = .0569; OHSU: 3.887 vs. 3.702, <i>p</i> = .048, adjusted-<i>p</i> = .288), <i>FLT3</i> mutation (median-log2, OHSU: 3.905 vs. 3.670, <i>p</i> = .007, adjusted-<i>p</i> = .044), compared with patients carrying wild type genes (Figure 2B–F).</p><p>Survival analyses showed that the overall survival (OS) of <i>MTAP</i>-low patients was significantly shorter than that of unaltered/high <i>MTAP</i> patients (<i>MTAP</i>-low patients vs. <i>MTAP</i>- unaltered/high patients; median-OS [months]: TCGA: 7.5 vs. 20.5, <i>p </i>= .014; OHSU: 10.16 vs. 17.79, <i>p </i>= .02, Figure 3A,B). Additionally, the disease-free survival (DFS) of MTAP-low patients was significantly lower than <i>MTAP</i>-unaltered/high patients in the TCGA dataset (<i>MTAP</i>-low patients (<i>n</i> = 18) vs. <i>MTAP</i>-unaltered/high patients (<i>n</i> = 153); median-DFS (months): 8.200 vs. 17.00, <i>p </i>= .017, Figure 3C). The OHSU dataset does not contain DFS data. We also conducted survival analyses after the exclusion of patients with AML M3, and patients with no available FAB data, due to the favourable prognosis of all-trans retinoic acid therapy. <i>MTAP</i>-low patients still have worse outcomes compared with <i>MTAP</i>-unaltered/high patients (TCGA: <i>MTAP</i>-low patients (<i>n</i> = 16) vs. <i>MTAP</i>-unaltered/high patients (<i>n</i> = 139); median OS (months): 7.200 vs. 17.40, <i>p </i>= 0.004, OHSU: <i>MTAP</i>-low patients (<i>n</i> = 50) vs. <i>MTAP</i>-unaltered/high patients (<i>n</i> = 349); 10.16 vs. 15.52, <i>p </i>= 0.035, Figure 3D,E). Multivariable analysis (cox-regression model) showed that <i>MTAP</i> low expression is significantly associated with OS (TCGA: <i>p </i>= 0.026; OHSU: <i>p </i>= 0.031) when adjusted by age, <i>DNMT3A-</i>mutation, <i>TP53-</i>mutation, <i>FLT3-</i>mutation (Table 1).</p><p>When comparing <i>MTAP</i> expression at different disease statuses in the OHSU dataset (initial diagnosis, remission, residual and relapse), we found <i>MTAP</i> expression levels were significantly higher at diagnosis (<i>n</i> = 443) than at remission (<i>n</i> = 25, median-log2: 3.855 vs. 3.073, <i>p </i>< .001, Figure 3F) or at residual disease (<i>n</i> = 129, median-log2: 3.855 vs. 3.491, <i>p</i> < .001, Figure 3G). <i>MTAP</i> expression was significantly higher at relapse (<i>n</i> = 36) than at remission (<i>n</i> = 25) (median-log2: 3.938 vs 3.073, <i>p </i>= .003, Figure 3H) and at residual disease (<i>n</i> = 129) (median-log2: 3.938 vs. 3.491, <i>p </i>= .002, Figure 3I). Consistently, <i>MTAP</i> expression levels were significantly higher in initial diagnosis compared with that in patients with residual disease when comparing samples from the same patients (<i>n</i> = 12, <i>p</i> = .001, Figure 3J).</p><p>Studies using synthetic lethal screens have shown that <i>MTAP</i>-deleted cells exhibit higher sensitivity to downregulation of PRMT5. <i>MTAP</i>-deleted cancer cells are particularly vulnerable to further inhibition of PRMT5 by the MTA-cooperative PRMT5 inhibitor MRTX1719.<span><sup>2</sup></span> This therapeutic approach selectively inhibits the PRMT5-MTA complex in <i>MTAP</i>-deficient cells.</p><p>MTA is generated through polyamine synthesis in which arginine is metabolized into ornithine and then into polyamines. Polyamine metabolism plays a key role in leukaemia stem cell survival and presents a potential therapeutic target in AML.<span><sup>10</sup></span> It is plausible that MTA accumulation plays an important metabolic vulnerability in AML cells, and thus MTA levels should be evaluated in patients with AML. Therapeutic strategies that are proven effective in <i>MTAP</i>-deleted cancers such as PRMT5 inhibitors and MTA-cooperative PRMT5 inhibitors should be investigated in the context of low MTA AML.</p><p>Altogether, our study reveals the association between low <i>MTAP</i> expression and shorter overall survival and the absence of <i>NPM1</i> mutation in patients with AML. Whether this is a causative association, what underlying mechanism of unfavourable clinical outcomes in patients with low <i>MTAP</i> expression, and whether <i>MTAP</i> low expression may lead to enhanced sensitivity to PRMT5 inhibitors remain to be studied.</p><p>Yiyu Xiao and Qianqian Peng: data analysis, validation and visualization, writing-original draft, reviewing-editing and methodology. Advaith Maya Sanjeev Kumar: data curation, analyses and validation, methodology. Houda Alachkar: conceptualization, resources, supervision, funding, validation, writing original draft, project administration, writing review and editing. All authors contributed to the article and approved the submitted version.</p><p>The authors declare no conflict of interest.</p><p>This study was supported by the University of Southern California Grant no. NIH-NCI 1R01CA248381-01A1 and National Institutes of Health (NIH) Grant no. 5P30CA014089-45.</p><p>Ethical approval was not required for the studies involving humans because this study was conducted on a publicly available dataset. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.</p>","PeriodicalId":10189,"journal":{"name":"Clinical and Translational Medicine","volume":"14 9","pages":""},"PeriodicalIF":7.9000,"publicationDate":"2024-09-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ctm2.70015","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.70015","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Dear Editor,
Deletions of methylthioadenosine phosphorylase (MTAP) are frequent in several malignancies and lead to 5′-deoxy-5′-methylthioadenosine (MTA) accumulation, competing with S-adenosylmethionine (SAM) for binding to Protein Arginine Methyltransferase 5 (PRMT5) and enhancing tumour sensitivity to PRMT5 inhibitors.1, 2 Although MTAP enzyme deficiency has been documented in acute myeloid leukaemia (AML), deletions of the MTAP gene have not been identified in this haematological malignancy. Here we evaluated MTAP downregulation in AML datasets (TCGA and OHSU)3-7 and its associations with clinical and molecular characteristics and patient's clinical outcome.
When comparing the MTAP expression between AML bone marrow (BM) (n = 542) and healthy BM (n = 73), different MTAP probes showed different results (MILE dataset,8 Figure 1A–F). However, when comparing the GTEx and TCGA datasets on UCSC Xena,9 we found higher MTAP expression in AML blood (n = 173) than normal blood samples (n = 337) (median-log2: 4.040 vs. −0.199, p = 6.596e−197, Figure 1G). Thirteen transcripts of MTAP were differentially expressed (Figure 1H). While only one deep deletion case was identified in AML in the TCGA dataset, using Z-score < −1 to define low expressor MTAP, we found 10.40% and 16.84% of cases have low MTAP expression in the TCGA and OHSU, respectively (Figure 1I).
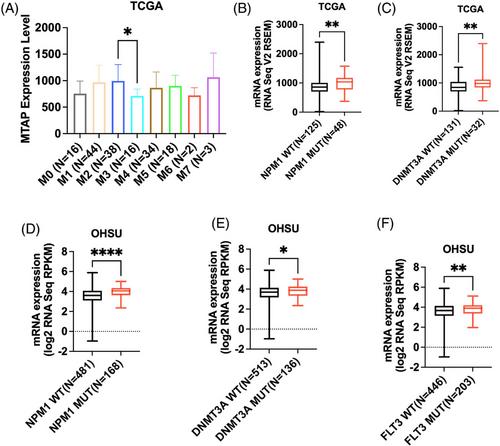
To investigate whether low expression of MTAP is associated with specific baseline clinical features in patients with AML, we compared the frequency of MTAP low expression according to diagnosis age, sex, BM blast percentage, white blood cell count, peripheral blasts percentage, cytogenetic risk and molecular risk (Tables S1 and S2). In the TCGA dataset, we found MTAP low expression to be more frequent in older patients (diagnosis age ≥ 65 years) than in younger patients (diagnosis age < 65 years) (18.87% vs. 6.67%, p = .027). MTAP expression levels were found to be lower in patients with AML M3 (n = 16) than AML M2 (n = 38) (p = .030, Figure 2A).
We also assessed the association between MTAP low expression and AML molecular characteristics in terms of the presence of certain AML mutations (Tables S3 and S4). We compared the frequencies of FLT3, DNMT3A, NPM1, IDH2, IDH1 and TP53 mutations between low and unaltered/high MTAP patients. In OHSU, patients with MTAP low expression have a lower frequency of FLT3 mutations (17.3% vs. 32.1%, p = .036) and NPM1 mutation (3.8% vs. 30.6%, p < .001) compared with unaltered/high MTAP group. MTAP was expressed at significantly higher levels in patients with NPM1 mutation (median-log2, TCGA: 1037 vs. 857.5, p = .0018, adjusted-p = .0112; OHSU: 4.058 vs. 3.606, p < .001, adjusted-p < .001), DNMT3A mutation (median-log2, TCGA: 980.3 vs. 844.0, p = .0094, adjusted-p = .0569; OHSU: 3.887 vs. 3.702, p = .048, adjusted-p = .288), FLT3 mutation (median-log2, OHSU: 3.905 vs. 3.670, p = .007, adjusted-p = .044), compared with patients carrying wild type genes (Figure 2B–F).
Survival analyses showed that the overall survival (OS) of MTAP-low patients was significantly shorter than that of unaltered/high MTAP patients (MTAP-low patients vs. MTAP- unaltered/high patients; median-OS [months]: TCGA: 7.5 vs. 20.5, p = .014; OHSU: 10.16 vs. 17.79, p = .02, Figure 3A,B). Additionally, the disease-free survival (DFS) of MTAP-low patients was significantly lower than MTAP-unaltered/high patients in the TCGA dataset (MTAP-low patients (n = 18) vs. MTAP-unaltered/high patients (n = 153); median-DFS (months): 8.200 vs. 17.00, p = .017, Figure 3C). The OHSU dataset does not contain DFS data. We also conducted survival analyses after the exclusion of patients with AML M3, and patients with no available FAB data, due to the favourable prognosis of all-trans retinoic acid therapy. MTAP-low patients still have worse outcomes compared with MTAP-unaltered/high patients (TCGA: MTAP-low patients (n = 16) vs. MTAP-unaltered/high patients (n = 139); median OS (months): 7.200 vs. 17.40, p = 0.004, OHSU: MTAP-low patients (n = 50) vs. MTAP-unaltered/high patients (n = 349); 10.16 vs. 15.52, p = 0.035, Figure 3D,E). Multivariable analysis (cox-regression model) showed that MTAP low expression is significantly associated with OS (TCGA: p = 0.026; OHSU: p = 0.031) when adjusted by age, DNMT3A-mutation, TP53-mutation, FLT3-mutation (Table 1).
When comparing MTAP expression at different disease statuses in the OHSU dataset (initial diagnosis, remission, residual and relapse), we found MTAP expression levels were significantly higher at diagnosis (n = 443) than at remission (n = 25, median-log2: 3.855 vs. 3.073, p < .001, Figure 3F) or at residual disease (n = 129, median-log2: 3.855 vs. 3.491, p < .001, Figure 3G). MTAP expression was significantly higher at relapse (n = 36) than at remission (n = 25) (median-log2: 3.938 vs 3.073, p = .003, Figure 3H) and at residual disease (n = 129) (median-log2: 3.938 vs. 3.491, p = .002, Figure 3I). Consistently, MTAP expression levels were significantly higher in initial diagnosis compared with that in patients with residual disease when comparing samples from the same patients (n = 12, p = .001, Figure 3J).
Studies using synthetic lethal screens have shown that MTAP-deleted cells exhibit higher sensitivity to downregulation of PRMT5. MTAP-deleted cancer cells are particularly vulnerable to further inhibition of PRMT5 by the MTA-cooperative PRMT5 inhibitor MRTX1719.2 This therapeutic approach selectively inhibits the PRMT5-MTA complex in MTAP-deficient cells.
MTA is generated through polyamine synthesis in which arginine is metabolized into ornithine and then into polyamines. Polyamine metabolism plays a key role in leukaemia stem cell survival and presents a potential therapeutic target in AML.10 It is plausible that MTA accumulation plays an important metabolic vulnerability in AML cells, and thus MTA levels should be evaluated in patients with AML. Therapeutic strategies that are proven effective in MTAP-deleted cancers such as PRMT5 inhibitors and MTA-cooperative PRMT5 inhibitors should be investigated in the context of low MTA AML.
Altogether, our study reveals the association between low MTAP expression and shorter overall survival and the absence of NPM1 mutation in patients with AML. Whether this is a causative association, what underlying mechanism of unfavourable clinical outcomes in patients with low MTAP expression, and whether MTAP low expression may lead to enhanced sensitivity to PRMT5 inhibitors remain to be studied.
Yiyu Xiao and Qianqian Peng: data analysis, validation and visualization, writing-original draft, reviewing-editing and methodology. Advaith Maya Sanjeev Kumar: data curation, analyses and validation, methodology. Houda Alachkar: conceptualization, resources, supervision, funding, validation, writing original draft, project administration, writing review and editing. All authors contributed to the article and approved the submitted version.
The authors declare no conflict of interest.
This study was supported by the University of Southern California Grant no. NIH-NCI 1R01CA248381-01A1 and National Institutes of Health (NIH) Grant no. 5P30CA014089-45.
Ethical approval was not required for the studies involving humans because this study was conducted on a publicly available dataset. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
期刊介绍:
Clinical and Translational Medicine (CTM) is an international, peer-reviewed, open-access journal dedicated to accelerating the translation of preclinical research into clinical applications and fostering communication between basic and clinical scientists. It highlights the clinical potential and application of various fields including biotechnologies, biomaterials, bioengineering, biomarkers, molecular medicine, omics science, bioinformatics, immunology, molecular imaging, drug discovery, regulation, and health policy. With a focus on the bench-to-bedside approach, CTM prioritizes studies and clinical observations that generate hypotheses relevant to patients and diseases, guiding investigations in cellular and molecular medicine. The journal encourages submissions from clinicians, researchers, policymakers, and industry professionals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


