Long guidewire peripheral intravenous catheters in emergency departments for management of difficult intravenous access: A multicenter, pragmatic, randomized controlled trial.
Hui Grace Xu, Amanda Corley, Emily R Young, Anna Doubrovsky, Robert S Ware, Clifford Afoakwah, Carrie Wang, Scott Stirling, Nicole Marsh
{"title":"Long guidewire peripheral intravenous catheters in emergency departments for management of difficult intravenous access: A multicenter, pragmatic, randomized controlled trial.","authors":"Hui Grace Xu, Amanda Corley, Emily R Young, Anna Doubrovsky, Robert S Ware, Clifford Afoakwah, Carrie Wang, Scott Stirling, Nicole Marsh","doi":"10.1111/acem.15004","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A quarter of patients who present to emergency departments (EDs) have difficult intravenous access (DIVA), making it challenging for clinicians to successfully place a peripheral intravenous catheter (PIVC). Some literature suggests that guidewire PIVC improves first-insertion success rate.</p><p><strong>Aim: </strong>The aim was to determine the clinical and cost-effectiveness of a novel long PIVC (5.8 cm) with a retractable coiled guidewire (GW-PIVC) for patients with DIVA, compared with standard care PIVCs.</p><p><strong>Methods: </strong>A pragmatic randomized controlled trial was conducted in two Australian EDs. Eligible participants were adults assessed as meeting DIVA criteria. Participants were randomized (1:1 ratio; stratified by hospital) to either GW-PIVC (long) or standard care group (short or long PIVC). The use of ultrasound was discretionary in the standard care group and was recommended in the GW-PIVC group due to the pragmatic design that was primarily testing the GW-PIVC rather than the ultrasound use. Primary outcome was first-insertion success and secondary outcomes included all-cause device failure, patient and staff satisfaction, and cost-effectiveness. The analysis was intention to treat.</p><p><strong>Results: </strong>A total of 446 participants were randomized and 409 received PIVCs. The use of GW-PIVC, compared with standard PIVC, had a lower first-insertion success rate (68% vs. 77%, odds ratio [OR] 0.65, 95% confidence interval [CI] 0.43-0.99, p < 0.05). There was no difference in PIVC failure (134.0 per 1000 catheter days [GW-PIVC] vs. 111.8 [standard PIVC] per 1000 catheter days, hazard ratio 1.18, 95% CI 0.72-1.95). Both participant (8/10 vs. 9/10, median difference [MD] -1.00, 95% CI -1.37 to -0.63) and clinician (8/10 vs. 10/10, MD -2.00, 95% CI -2.37 to -1.63) satisfaction was lower with GW-PIVCs compared with standard PIVCs. More nurses inserted standard PIVCs than GW-PIVCs (56.9% vs. 36.5%) and had less confidence in their ultrasound skills (28.0% vs. 46.6% self-claimed as advanced/expert users). The cost per participant of GW-PIVC insertions was 2.46 times greater than standard PIVC insertions ($AU80.24 vs. $AU32.57).</p><p><strong>Conclusions: </strong>GW-PIVCs had significantly lower first-insertion success and non-significantly higher all-cause catheter failure. Additional training and device design familiar to clinicians are vital factors to enhance the likelihood of successful future implementation of GW-PIVCs.</p>","PeriodicalId":7105,"journal":{"name":"Academic Emergency Medicine","volume":" ","pages":"1223-1232"},"PeriodicalIF":3.2000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11649600/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Academic Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/acem.15004","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/9 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A quarter of patients who present to emergency departments (EDs) have difficult intravenous access (DIVA), making it challenging for clinicians to successfully place a peripheral intravenous catheter (PIVC). Some literature suggests that guidewire PIVC improves first-insertion success rate.
Aim: The aim was to determine the clinical and cost-effectiveness of a novel long PIVC (5.8 cm) with a retractable coiled guidewire (GW-PIVC) for patients with DIVA, compared with standard care PIVCs.
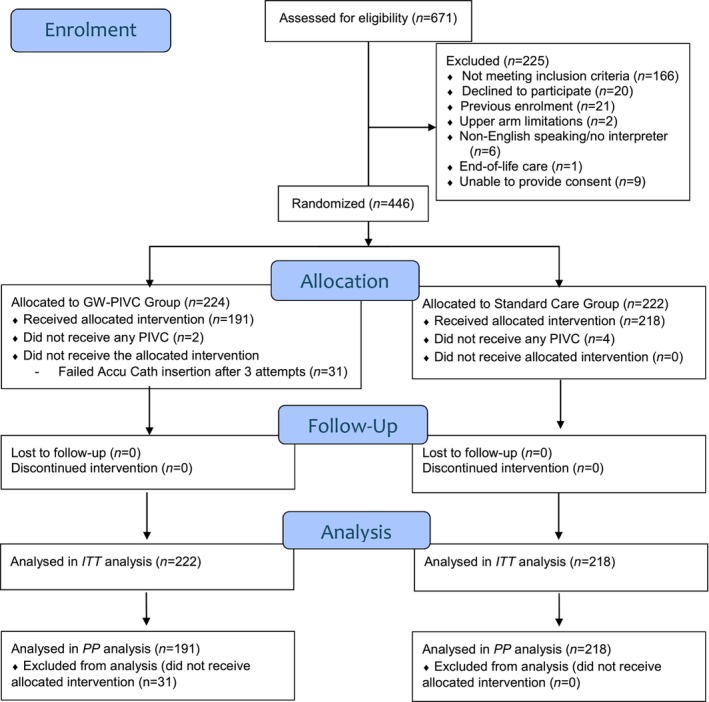
Methods: A pragmatic randomized controlled trial was conducted in two Australian EDs. Eligible participants were adults assessed as meeting DIVA criteria. Participants were randomized (1:1 ratio; stratified by hospital) to either GW-PIVC (long) or standard care group (short or long PIVC). The use of ultrasound was discretionary in the standard care group and was recommended in the GW-PIVC group due to the pragmatic design that was primarily testing the GW-PIVC rather than the ultrasound use. Primary outcome was first-insertion success and secondary outcomes included all-cause device failure, patient and staff satisfaction, and cost-effectiveness. The analysis was intention to treat.
Results: A total of 446 participants were randomized and 409 received PIVCs. The use of GW-PIVC, compared with standard PIVC, had a lower first-insertion success rate (68% vs. 77%, odds ratio [OR] 0.65, 95% confidence interval [CI] 0.43-0.99, p < 0.05). There was no difference in PIVC failure (134.0 per 1000 catheter days [GW-PIVC] vs. 111.8 [standard PIVC] per 1000 catheter days, hazard ratio 1.18, 95% CI 0.72-1.95). Both participant (8/10 vs. 9/10, median difference [MD] -1.00, 95% CI -1.37 to -0.63) and clinician (8/10 vs. 10/10, MD -2.00, 95% CI -2.37 to -1.63) satisfaction was lower with GW-PIVCs compared with standard PIVCs. More nurses inserted standard PIVCs than GW-PIVCs (56.9% vs. 36.5%) and had less confidence in their ultrasound skills (28.0% vs. 46.6% self-claimed as advanced/expert users). The cost per participant of GW-PIVC insertions was 2.46 times greater than standard PIVC insertions ($AU80.24 vs. $AU32.57).
Conclusions: GW-PIVCs had significantly lower first-insertion success and non-significantly higher all-cause catheter failure. Additional training and device design familiar to clinicians are vital factors to enhance the likelihood of successful future implementation of GW-PIVCs.
期刊介绍:
Academic Emergency Medicine (AEM) is the official monthly publication of the Society for Academic Emergency Medicine (SAEM) and publishes information relevant to the practice, educational advancements, and investigation of emergency medicine. It is the second-largest peer-reviewed scientific journal in the specialty of emergency medicine.
The goal of AEM is to advance the science, education, and clinical practice of emergency medicine, to serve as a voice for the academic emergency medicine community, and to promote SAEM''s goals and objectives. Members and non-members worldwide depend on this journal for translational medicine relevant to emergency medicine, as well as for clinical news, case studies and more.
Each issue contains information relevant to the research, educational advancements, and practice in emergency medicine. Subject matter is diverse, including preclinical studies, clinical topics, health policy, and educational methods. The research of SAEM members contributes significantly to the scientific content and development of the journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


