Zongsheng Hu, Radhe Mohan, Yan Chu, Xiaochun Wang, Peter S N van Rossum, Yiqing Chen, Madison E Grayson, Angela G Gearhardt, Clemens Grassberger, Degui Zhi, Brian P Hobbs, Steven H Lin, Wenhua Cao
{"title":"Clinical Translation of a Deep Learning Model of Radiation-Induced Lymphopenia for Esophageal Cancer.","authors":"Zongsheng Hu, Radhe Mohan, Yan Chu, Xiaochun Wang, Peter S N van Rossum, Yiqing Chen, Madison E Grayson, Angela G Gearhardt, Clemens Grassberger, Degui Zhi, Brian P Hobbs, Steven H Lin, Wenhua Cao","doi":"10.1016/j.ijpt.2024.100624","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Radiation-induced lymphopenia is a common immune toxicity that adversely impacts treatment outcomes. We report here our approach to translate a deep-learning (DL) model developed to predict severe lymphopenia risk among esophageal cancer into a strategy for incorporating the immune system as an organ-at-risk (iOAR) to mitigate the risk.</p><p><strong>Materials and methods: </strong>We conducted \"virtual clinical trials\" utilizing retrospective data for 10 intensity-modulated radiation therapy (IMRT) and 10 passively-scattered proton therapy (PSPT) esophageal cancer patients. For each patient, additional treatment plans of the modality other than the original were created employing standard-of-care (SOC) dose constraints. Predicted values of absolute lymphocyte count (ALC) nadir for all plans were estimated using a previously-developed DL model. The model also yielded the relative magnitudes of contributions of iOARs dosimetric factors to ALC nadir, which were used to compute iOARs dose-volume constraints, which were incorporated into optimization criteria to produce \"IMRT-enhanced\" and \"intensity-modulated proton therapy (IMPT)-enhanced\" plans.</p><p><strong>Results: </strong>Model-predicted ALC nadir for the original IMRT (IMRT-SOC) and PSPT plans agreed well with actual values. IMPT-SOC showed greater immune sparing vs IMRT and PSPT. The average mean body doses were 13.10 Gy vs 7.62 Gy for IMRT-SOC vs IMPT-SOC for patients treated with IMRT-SOC; and 8.08 Gy vs 6.68 Gy for PSPT vs IMPT-SOC for patients treated with PSPT. For IMRT patients, the average predicted ALC nadir of IMRT-SOC, IMRT-enhanced, IMPT-SOC, and IMPT-enhanced was 281, 327, 351, and 392 cells/µL, respectively. For PSPT patients, the average predicted ALC nadir of PSPT, IMPT-SOC, and IMPT-enhanced was 258, 316, and 350 cells/µL, respectively. Enhanced plans achieved higher predicted ALC nadir, with an average improvement of 40.8 cells/µL (20.6%).</p><p><strong>Conclusion: </strong>The proposed DL model-guided strategy to incorporate the immune system as iOAR in IMRT and IMPT optimization has the potential for radiation-induced lymphopenia mitigation. A prospective clinical trial is planned.</p>","PeriodicalId":36923,"journal":{"name":"International Journal of Particle Therapy","volume":"13 ","pages":"100624"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11369390/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Particle Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.ijpt.2024.100624","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Radiation-induced lymphopenia is a common immune toxicity that adversely impacts treatment outcomes. We report here our approach to translate a deep-learning (DL) model developed to predict severe lymphopenia risk among esophageal cancer into a strategy for incorporating the immune system as an organ-at-risk (iOAR) to mitigate the risk.
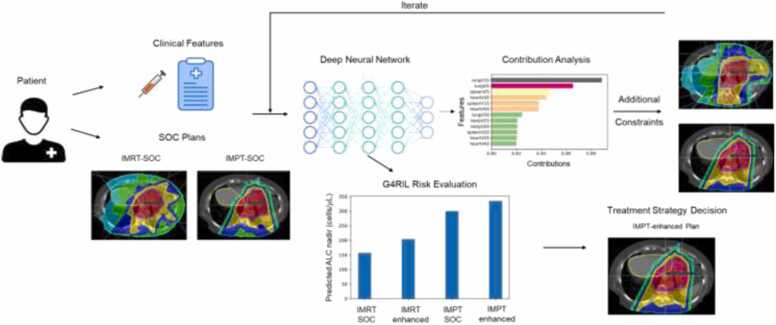
Materials and methods: We conducted "virtual clinical trials" utilizing retrospective data for 10 intensity-modulated radiation therapy (IMRT) and 10 passively-scattered proton therapy (PSPT) esophageal cancer patients. For each patient, additional treatment plans of the modality other than the original were created employing standard-of-care (SOC) dose constraints. Predicted values of absolute lymphocyte count (ALC) nadir for all plans were estimated using a previously-developed DL model. The model also yielded the relative magnitudes of contributions of iOARs dosimetric factors to ALC nadir, which were used to compute iOARs dose-volume constraints, which were incorporated into optimization criteria to produce "IMRT-enhanced" and "intensity-modulated proton therapy (IMPT)-enhanced" plans.
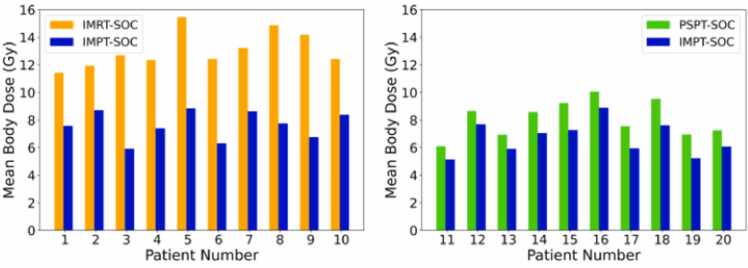
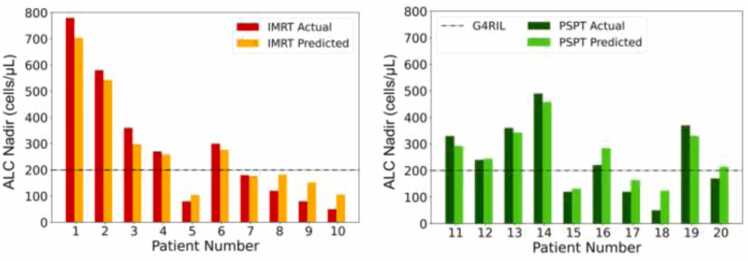
Results: Model-predicted ALC nadir for the original IMRT (IMRT-SOC) and PSPT plans agreed well with actual values. IMPT-SOC showed greater immune sparing vs IMRT and PSPT. The average mean body doses were 13.10 Gy vs 7.62 Gy for IMRT-SOC vs IMPT-SOC for patients treated with IMRT-SOC; and 8.08 Gy vs 6.68 Gy for PSPT vs IMPT-SOC for patients treated with PSPT. For IMRT patients, the average predicted ALC nadir of IMRT-SOC, IMRT-enhanced, IMPT-SOC, and IMPT-enhanced was 281, 327, 351, and 392 cells/µL, respectively. For PSPT patients, the average predicted ALC nadir of PSPT, IMPT-SOC, and IMPT-enhanced was 258, 316, and 350 cells/µL, respectively. Enhanced plans achieved higher predicted ALC nadir, with an average improvement of 40.8 cells/µL (20.6%).
Conclusion: The proposed DL model-guided strategy to incorporate the immune system as iOAR in IMRT and IMPT optimization has the potential for radiation-induced lymphopenia mitigation. A prospective clinical trial is planned.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


