Aldin Malkoc, Lana Mamoun, Kendall Vignaroli, Harpreet Gill, Amira Barmanwalla, Alexander Phan, Amanda Daoud, Alexandra Nguyen, Brandon Woodward
{"title":"Conservative Treatment of Empyema Formation Following Intrathoracic Rib Fixation With Antibiotics and Tissue Plasminogen Activator/Dornase.","authors":"Aldin Malkoc, Lana Mamoun, Kendall Vignaroli, Harpreet Gill, Amira Barmanwalla, Alexander Phan, Amanda Daoud, Alexandra Nguyen, Brandon Woodward","doi":"10.14740/jmc4267","DOIUrl":null,"url":null,"abstract":"<p><p>Rib plating is a recommended intervention for patients with multiple rib fractures or flail chest to improve shortness of breath, significantly reduce pain, and shorten the length of hospital stay. Here, we report a unique and extremely rare finding in a patient with empyema following intrathoracic rib fixation. A 32-year-old male with a history of alcohol use disorder presented to the emergency department trauma bay after a motor vehicle accident. Computed tomography (CT) showed right hemopneumothorax and fourth to ninth rib fractures with displacement. The right fifth and sixth ribs were then plated using a titanium RibFix bridge, implanted intrathoracically along the posterior surface of the ribs. On postoperative day 11, the patient developed an empyema and a CT-guided drainage catheter was placed into the collection. The patient was given a 3-day course of tissue plasminogen activator (tPA) and DNase for the treatment of his empyema. On postoperative day 15, a repeat CT scan demonstrated significant improvement in the empyema with evidence of abscess resolution. Antibiotics were discontinued after a total of 7 days and the patient was discharged on postoperative day 20. This case report contributes information to the management of complications in intrathoracic rib fixation.</p>","PeriodicalId":101328,"journal":{"name":"Journal of medical cases","volume":"15 9","pages":"215-221"},"PeriodicalIF":0.9000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11349117/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of medical cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4267","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/10 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
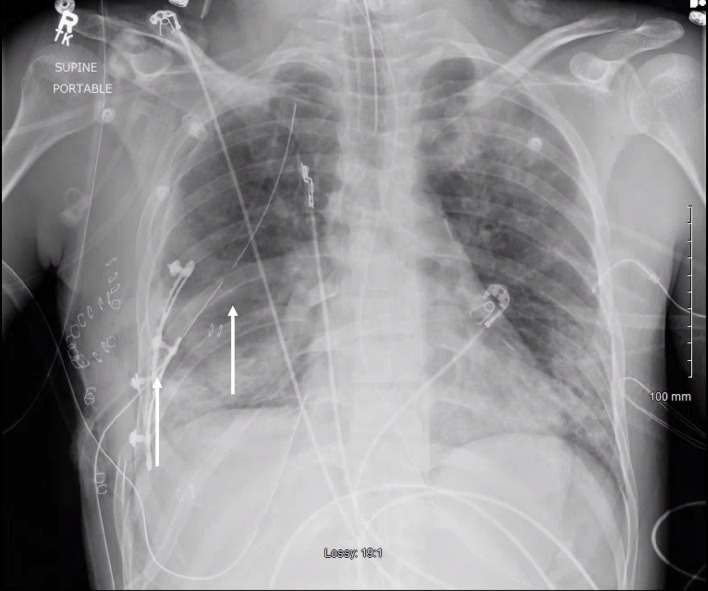
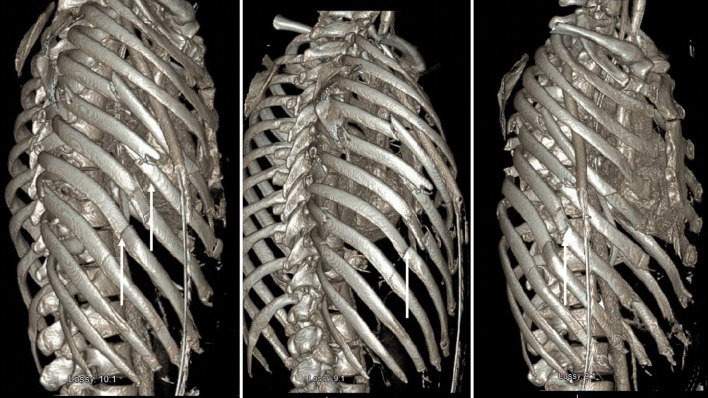
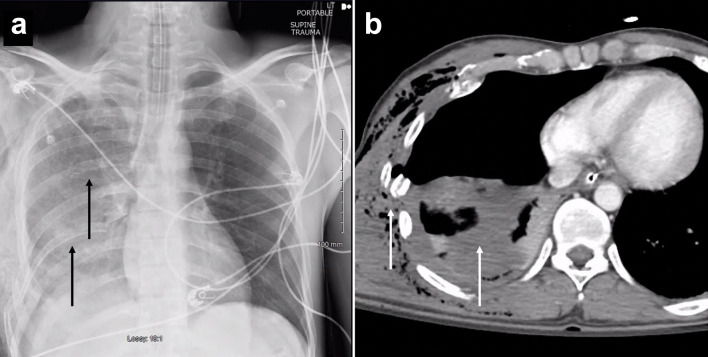
Rib plating is a recommended intervention for patients with multiple rib fractures or flail chest to improve shortness of breath, significantly reduce pain, and shorten the length of hospital stay. Here, we report a unique and extremely rare finding in a patient with empyema following intrathoracic rib fixation. A 32-year-old male with a history of alcohol use disorder presented to the emergency department trauma bay after a motor vehicle accident. Computed tomography (CT) showed right hemopneumothorax and fourth to ninth rib fractures with displacement. The right fifth and sixth ribs were then plated using a titanium RibFix bridge, implanted intrathoracically along the posterior surface of the ribs. On postoperative day 11, the patient developed an empyema and a CT-guided drainage catheter was placed into the collection. The patient was given a 3-day course of tissue plasminogen activator (tPA) and DNase for the treatment of his empyema. On postoperative day 15, a repeat CT scan demonstrated significant improvement in the empyema with evidence of abscess resolution. Antibiotics were discontinued after a total of 7 days and the patient was discharged on postoperative day 20. This case report contributes information to the management of complications in intrathoracic rib fixation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


