Nathan C Beckett, Jack Haglin, Paul Van Schuyver, Mark J Spangehl, Maziyar A Kalani, Mark K Lyons, Abhijith R Bathinin, Joshua S Bingham
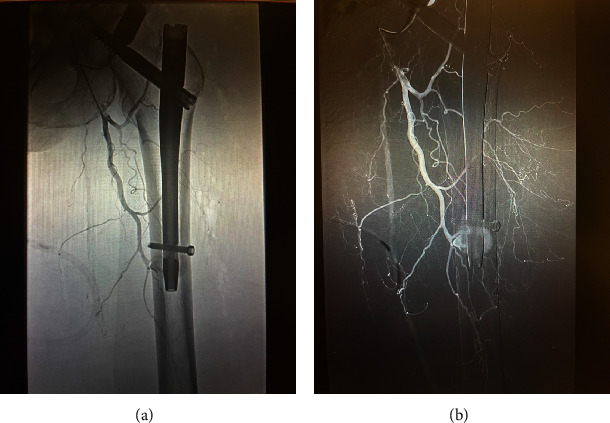
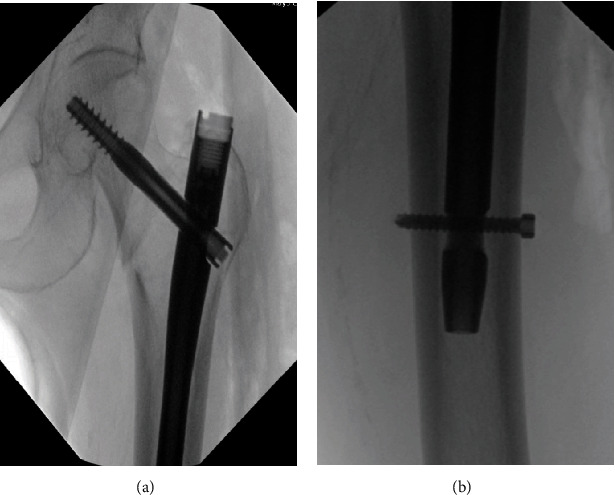
{"title":"Traumatic Disruption of Profunda Femoris Artery Branch Following Treatment of an Intertrochanteric Hip Fracture With a Cephalomedullary Nail.","authors":"Nathan C Beckett, Jack Haglin, Paul Van Schuyver, Mark J Spangehl, Maziyar A Kalani, Mark K Lyons, Abhijith R Bathinin, Joshua S Bingham","doi":"10.1155/2024/5590091","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Surgical management of intertrochanteric hip fractures is a common surgery with low rates of intraoperative complications. Vascular injuries are exceptionally rare when placing an intramedullary nail without open reduction. There are very few reported cases of direct arterial injury and active bleed at the level of the distal interlocking screw following closed reduction and intramedullary nailing of a hip fracture. We report one such case. <b>Case Presentation:</b> An 88-year-old female presented to the emergency department with a left intertrochanteric hip fracture. Closed reduction with a cephalomedullary nail fixation of the left hip fracture occurred as planned without any obvious intraoperative technical issues. The patient remained stable intraoperatively. No open reduction was required. Postoperatively, the patient developed hemorrhagic shock and required massive transfusion protocol. Angiography demonstrated an intramuscular hematoma at the level of the distal intramedullary nail interlocking screw with active extravasation. The patient subsequently required embolization. Nine days following surgery, she began Eliquis for DVT prophylaxis and was ambulating independently with signs of hematoma resolution. <b>Discussion:</b> Profunda femoris artery injury can stem from various mechanisms during surgery. Atherosclerosis places patients at a higher risk of complication due to rigid vessels. In this case, it is believed that drilling beyond the medial femoral cortex led to the arterial injury. <b>Conclusion:</b> Care should be taken to prevent drills from plunging beyond the medial femoral cortex during surgery. Cautious observation of patient's vitals and clinical course can allow for early detection of vascular complication.</p>","PeriodicalId":30287,"journal":{"name":"Case Reports in Orthopedics","volume":"2024 ","pages":"5590091"},"PeriodicalIF":0.6000,"publicationDate":"2024-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11357815/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/5590091","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Surgical management of intertrochanteric hip fractures is a common surgery with low rates of intraoperative complications. Vascular injuries are exceptionally rare when placing an intramedullary nail without open reduction. There are very few reported cases of direct arterial injury and active bleed at the level of the distal interlocking screw following closed reduction and intramedullary nailing of a hip fracture. We report one such case. Case Presentation: An 88-year-old female presented to the emergency department with a left intertrochanteric hip fracture. Closed reduction with a cephalomedullary nail fixation of the left hip fracture occurred as planned without any obvious intraoperative technical issues. The patient remained stable intraoperatively. No open reduction was required. Postoperatively, the patient developed hemorrhagic shock and required massive transfusion protocol. Angiography demonstrated an intramuscular hematoma at the level of the distal intramedullary nail interlocking screw with active extravasation. The patient subsequently required embolization. Nine days following surgery, she began Eliquis for DVT prophylaxis and was ambulating independently with signs of hematoma resolution. Discussion: Profunda femoris artery injury can stem from various mechanisms during surgery. Atherosclerosis places patients at a higher risk of complication due to rigid vessels. In this case, it is believed that drilling beyond the medial femoral cortex led to the arterial injury. Conclusion: Care should be taken to prevent drills from plunging beyond the medial femoral cortex during surgery. Cautious observation of patient's vitals and clinical course can allow for early detection of vascular complication.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


