{"title":"Transcatheter Arterial Embolization for Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Retrospective Study of 44 Patients.","authors":"Takatoshi Kubo, Masahiko Shibuya, Koichi Miyazaki, Yusuke Tsuji, Masaya Nakata, Atsuhiko Kawabe, Takashi Nakasone, Nobuaki Sakai, Yuji Okuno","doi":"10.1007/s00270-024-03842-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To investigate the preliminary treatment outcomes of transcatheter arterial embolization (TAE) for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS).</p><p><strong>Materials and methods: </strong>This retrospective study included patients with refractory CP/CPPS who underwent TAE between April 2022 and February 2023. All patients had persistent pelvic pain for at least 3 months, a total score of at least 15 on the NIH-Chronic Prostatitis Symptom Index (NIH-CPSI), and lacked evidence of infection. All procedures were performed by injecting imipenem/cilastatin sodium (IPM/CS) from bilateral prostatic arteries ± internal pudendal arteries. NIH-CPSI, pain numeric rating scale (NRS), and complications were evaluated at 1, 3, and 6 months after the initial TAE and at the final follow-up.</p><p><strong>Results: </strong>Out of 48 patients, 44 were included in this study, with four excluded because of loss of follow-up. No severe procedure-related complications were observed. Pretreatment and post-treatment evaluations at 1, 3, and 6 months after the initial TAE and at the final follow-up (mean 16.6 months) revealed a decrease in the mean NIH-CPSI scores from 27 ± 6 to 21 ± 8, 20 ± 9, 17 ± 9, and 18 ± 9, respectively (all P < 0.001). Pain NRS scores were also decreased from 7.0 ± 1.6 to 4.8 ± 2.5, 4.1 ± 2.6, 3.7 ± 2.4, and 3.4 ± 2.3, respectively (all P < 0.001). The proportions of clinical success, defined as a reduction of at least 6 points from baseline in the NIH-CPSI, at 6 months after TAE and at the final follow-up were 70 and 64%, respectively.</p><p><strong>Conclusions: </strong>This study provides evidence of the feasibility of TAE using IPM/CS for CP/CPPS, suggesting both symptomatic improvement and safety.</p>","PeriodicalId":9591,"journal":{"name":"CardioVascular and Interventional Radiology","volume":null,"pages":null},"PeriodicalIF":2.8000,"publicationDate":"2024-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CardioVascular and Interventional Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00270-024-03842-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To investigate the preliminary treatment outcomes of transcatheter arterial embolization (TAE) for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS).
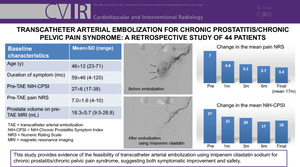
Materials and methods: This retrospective study included patients with refractory CP/CPPS who underwent TAE between April 2022 and February 2023. All patients had persistent pelvic pain for at least 3 months, a total score of at least 15 on the NIH-Chronic Prostatitis Symptom Index (NIH-CPSI), and lacked evidence of infection. All procedures were performed by injecting imipenem/cilastatin sodium (IPM/CS) from bilateral prostatic arteries ± internal pudendal arteries. NIH-CPSI, pain numeric rating scale (NRS), and complications were evaluated at 1, 3, and 6 months after the initial TAE and at the final follow-up.
Results: Out of 48 patients, 44 were included in this study, with four excluded because of loss of follow-up. No severe procedure-related complications were observed. Pretreatment and post-treatment evaluations at 1, 3, and 6 months after the initial TAE and at the final follow-up (mean 16.6 months) revealed a decrease in the mean NIH-CPSI scores from 27 ± 6 to 21 ± 8, 20 ± 9, 17 ± 9, and 18 ± 9, respectively (all P < 0.001). Pain NRS scores were also decreased from 7.0 ± 1.6 to 4.8 ± 2.5, 4.1 ± 2.6, 3.7 ± 2.4, and 3.4 ± 2.3, respectively (all P < 0.001). The proportions of clinical success, defined as a reduction of at least 6 points from baseline in the NIH-CPSI, at 6 months after TAE and at the final follow-up were 70 and 64%, respectively.
Conclusions: This study provides evidence of the feasibility of TAE using IPM/CS for CP/CPPS, suggesting both symptomatic improvement and safety.
期刊介绍:
CardioVascular and Interventional Radiology (CVIR) is the official journal of the Cardiovascular and Interventional Radiological Society of Europe, and is also the official organ of a number of additional distinguished national and international interventional radiological societies. CVIR publishes double blinded peer-reviewed original research work including clinical and laboratory investigations, technical notes, case reports, works in progress, and letters to the editor, as well as review articles, pictorial essays, editorials, and special invited submissions in the field of vascular and interventional radiology. Beside the communication of the latest research results in this field, it is also the aim of CVIR to support continuous medical education. Articles that are accepted for publication are done so with the understanding that they, or their substantive contents, have not been and will not be submitted to any other publication.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


