Georgios Vlasakakis, Michael T. McCabe, Yu Liu Ho, Geraldine Ferron-Brady, Paul Martin, Darren Bentley, Catherine Ellis, Mary Antonysamy, Sandra A. G. Visser
{"title":"Momelotinib: Mechanism of action, clinical, and translational science","authors":"Georgios Vlasakakis, Michael T. McCabe, Yu Liu Ho, Geraldine Ferron-Brady, Paul Martin, Darren Bentley, Catherine Ellis, Mary Antonysamy, Sandra A. G. Visser","doi":"10.1111/cts.70018","DOIUrl":null,"url":null,"abstract":"<p>Myelofibrosis is a chronic myeloproliferative disorder characterized by bone marrow fibrosis, splenomegaly, anemia, and constitutional symptoms, with a median survival of ≈6 years from diagnosis. While currently approved Janus kinase (JAK) inhibitors (ruxolitinib, fedratinib) improve splenomegaly and symptoms, most can exacerbate myelofibrosis-related anemia, a negative prognostic factor for survival. Momelotinib is a novel JAK1/JAK2/activin A receptor type 1 (ACVR1) inhibitor approved in the US, European Union, and the UK and is the first JAK inhibitor indicated specifically for patients with myelofibrosis with anemia. Momelotinib not only addresses the splenomegaly and symptoms associated with myelofibrosis by suppressing the hyperactive JAK–STAT (signal transducer and activator of transcription) pathway but also improves anemia and reduces transfusion dependency through ACVR1 inhibition. The recommended dose of momelotinib is 200 mg orally once daily, which was established after review of safety, efficacy, pharmacokinetic, and pharmacodynamic data. Momelotinib is metabolized primarily by CYP3A4 and excreted as metabolites in feces and urine. Steady-state maximum concentration is 479 ng/mL (CV%, 61%), with a mean AUC<sub>tau</sub> of 3288 ng.h/mL (CV%, 60%); its major metabolite, M21, is active (≈40% of pharmacological activity of parent), with a metabolite-to-parent AUC ratio of 1.4–2.1. This review describes momelotinib's mechanism of action, detailing how the JAK–STAT pathway is involved in myelofibrosis pathogenesis and ACVR1 inhibition decreases hepcidin, leading to improved erythropoiesis. Additionally, it summarizes the pivotal studies and data that informed the recommended dosage and risk/benefit assessment.</p>","PeriodicalId":50610,"journal":{"name":"Cts-Clinical and Translational Science","volume":"17 8","pages":""},"PeriodicalIF":3.1000,"publicationDate":"2024-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cts.70018","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cts-Clinical and Translational Science","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cts.70018","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
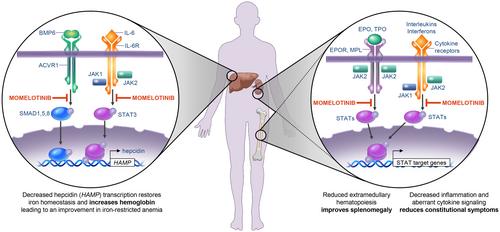
Myelofibrosis is a chronic myeloproliferative disorder characterized by bone marrow fibrosis, splenomegaly, anemia, and constitutional symptoms, with a median survival of ≈6 years from diagnosis. While currently approved Janus kinase (JAK) inhibitors (ruxolitinib, fedratinib) improve splenomegaly and symptoms, most can exacerbate myelofibrosis-related anemia, a negative prognostic factor for survival. Momelotinib is a novel JAK1/JAK2/activin A receptor type 1 (ACVR1) inhibitor approved in the US, European Union, and the UK and is the first JAK inhibitor indicated specifically for patients with myelofibrosis with anemia. Momelotinib not only addresses the splenomegaly and symptoms associated with myelofibrosis by suppressing the hyperactive JAK–STAT (signal transducer and activator of transcription) pathway but also improves anemia and reduces transfusion dependency through ACVR1 inhibition. The recommended dose of momelotinib is 200 mg orally once daily, which was established after review of safety, efficacy, pharmacokinetic, and pharmacodynamic data. Momelotinib is metabolized primarily by CYP3A4 and excreted as metabolites in feces and urine. Steady-state maximum concentration is 479 ng/mL (CV%, 61%), with a mean AUCtau of 3288 ng.h/mL (CV%, 60%); its major metabolite, M21, is active (≈40% of pharmacological activity of parent), with a metabolite-to-parent AUC ratio of 1.4–2.1. This review describes momelotinib's mechanism of action, detailing how the JAK–STAT pathway is involved in myelofibrosis pathogenesis and ACVR1 inhibition decreases hepcidin, leading to improved erythropoiesis. Additionally, it summarizes the pivotal studies and data that informed the recommended dosage and risk/benefit assessment.
期刊介绍:
Clinical and Translational Science (CTS), an official journal of the American Society for Clinical Pharmacology and Therapeutics, highlights original translational medicine research that helps bridge laboratory discoveries with the diagnosis and treatment of human disease. Translational medicine is a multi-faceted discipline with a focus on translational therapeutics. In a broad sense, translational medicine bridges across the discovery, development, regulation, and utilization spectrum. Research may appear as Full Articles, Brief Reports, Commentaries, Phase Forwards (clinical trials), Reviews, or Tutorials. CTS also includes invited didactic content that covers the connections between clinical pharmacology and translational medicine. Best-in-class methodologies and best practices are also welcomed as Tutorials. These additional features provide context for research articles and facilitate understanding for a wide array of individuals interested in clinical and translational science. CTS welcomes high quality, scientifically sound, original manuscripts focused on clinical pharmacology and translational science, including animal, in vitro, in silico, and clinical studies supporting the breadth of drug discovery, development, regulation and clinical use of both traditional drugs and innovative modalities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


