{"title":"A 3D-CT Study of the Cortical Bone Trajectory Screw Placement Parameters Based on Lumbar CT.","authors":"Weibo Zeng, Shengxuan Hu, Zhemin Zhu, Shuai Wang, Lijun Guo, Benchao Shi","doi":"10.1111/os.14202","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The cortical bone trajectory (CBT) technology is an effective substitute for traditional pedicle screw (PS) technology. However, there is still controversy about the CBT screw technology placement strategy. The objective of this study was to simulate cortical screw placement with the help of three-dimensional (3D) software, to discuss the differences in screws between genders and vertebral segments, and to explore a safer and more efficient strategy for cortical screw placement.</p><p><strong>Methods: </strong>Mimics Medical software was used to construct a 3D model of the lumbar spine, and the placement of CBT screws was simulated. The volume of each vertebral body from L1 to L5, the pedicle isthmus height (IH), the pedicle isthmus width (IW), and the sagittal vertebral distance (SAVD) were measured. The transverse distance (TD) and the longitudinal distance (LD) between the ideal starting point (SP) and the clinical SP (the intersection Q of the midline of the superior articular process and the horizontal line 1 mm below the transverse process) were measured. The cephalad angle (CA), lateral angle (LA), maximum screw diameter (MSD), maximum screw length (MSL) of each trajectory of the L1 to L5 vertebral bodies, and the percentage of the screw insertion depth (PSID) into the vertebral body were measured. Data were statistically analyzed using Student's t-test, one-way analysis of variance (ANOVA), and Tukey's test.</p><p><strong>Results: </strong>Vertebral anatomical parameters and CBT screw parameters differed between males and females. Female patients had lower IH, IW, SAVD, CA, LA, MSD, and MSL than males. IH was greatest in L1 (male, 17.81 mm; female, 16.12 mm) and the smallest in L5 (male, 14.11 mm; female, 13.05 mm). IW was smallest in L1 (male, 8.89 mm; female, 7.37 mm) and greatest in L5 (male, 16.59 mm; female, 15.43 mm). The MSD of males was smallest in L1 (6.05 mm) and greatest in L3 (7.06 mm); the MSD of females was smallest in L1 (5.13 mm) and greatest in L4 (6.64 mm). MSL was greatest at L3 (male, 33.63 mm; female, 32.28 mm) and smallest at L5 (male, 31.25 mm; female, 29.97 mm). CA was smallest in L1 (male, 22.80°; female, 21.92°) and greatest in L3 (male, 25.29°; female, 24.33°). LA was smallest in L1 (male 12.37°, female 11.27°) and greatest in L5 (male 13.56°, female 12.96°). Among the males, TD was smallest at L1 (-0.51 mm) and greatest at L5 (1.37 mm), while LD was greatest at L2 (3.46 mm) and smallest at L5 (2.40 mm). In females, TD was greatest at L1 (0.12 mm) and smallest at L3 (-0.51 mm), while LD was greatest at L1 (3.69 mm) and smallest at L5 (2.08 mm). In the overall sample, the incidence of SAVD and PSID gradually increased from L1 to L5.</p><p><strong>Conclusion: </strong>The optimal screw placement strategy for CBT screws varies significantly according to sex and vertebral body segments, particularly noting the specificity of screw placement at L5. The optimal screw placement strategy should be selected based on the patient's sex and segment characteristics before surgery to maximize the safety and accuracy of CBT screw placement.</p>","PeriodicalId":19566,"journal":{"name":"Orthopaedic Surgery","volume":" ","pages":"2771-2780"},"PeriodicalIF":1.8000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11541135/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Orthopaedic Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/os.14202","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/26 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The cortical bone trajectory (CBT) technology is an effective substitute for traditional pedicle screw (PS) technology. However, there is still controversy about the CBT screw technology placement strategy. The objective of this study was to simulate cortical screw placement with the help of three-dimensional (3D) software, to discuss the differences in screws between genders and vertebral segments, and to explore a safer and more efficient strategy for cortical screw placement.
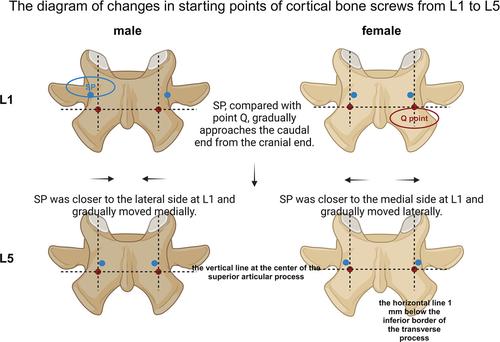
Methods: Mimics Medical software was used to construct a 3D model of the lumbar spine, and the placement of CBT screws was simulated. The volume of each vertebral body from L1 to L5, the pedicle isthmus height (IH), the pedicle isthmus width (IW), and the sagittal vertebral distance (SAVD) were measured. The transverse distance (TD) and the longitudinal distance (LD) between the ideal starting point (SP) and the clinical SP (the intersection Q of the midline of the superior articular process and the horizontal line 1 mm below the transverse process) were measured. The cephalad angle (CA), lateral angle (LA), maximum screw diameter (MSD), maximum screw length (MSL) of each trajectory of the L1 to L5 vertebral bodies, and the percentage of the screw insertion depth (PSID) into the vertebral body were measured. Data were statistically analyzed using Student's t-test, one-way analysis of variance (ANOVA), and Tukey's test.
Results: Vertebral anatomical parameters and CBT screw parameters differed between males and females. Female patients had lower IH, IW, SAVD, CA, LA, MSD, and MSL than males. IH was greatest in L1 (male, 17.81 mm; female, 16.12 mm) and the smallest in L5 (male, 14.11 mm; female, 13.05 mm). IW was smallest in L1 (male, 8.89 mm; female, 7.37 mm) and greatest in L5 (male, 16.59 mm; female, 15.43 mm). The MSD of males was smallest in L1 (6.05 mm) and greatest in L3 (7.06 mm); the MSD of females was smallest in L1 (5.13 mm) and greatest in L4 (6.64 mm). MSL was greatest at L3 (male, 33.63 mm; female, 32.28 mm) and smallest at L5 (male, 31.25 mm; female, 29.97 mm). CA was smallest in L1 (male, 22.80°; female, 21.92°) and greatest in L3 (male, 25.29°; female, 24.33°). LA was smallest in L1 (male 12.37°, female 11.27°) and greatest in L5 (male 13.56°, female 12.96°). Among the males, TD was smallest at L1 (-0.51 mm) and greatest at L5 (1.37 mm), while LD was greatest at L2 (3.46 mm) and smallest at L5 (2.40 mm). In females, TD was greatest at L1 (0.12 mm) and smallest at L3 (-0.51 mm), while LD was greatest at L1 (3.69 mm) and smallest at L5 (2.08 mm). In the overall sample, the incidence of SAVD and PSID gradually increased from L1 to L5.
Conclusion: The optimal screw placement strategy for CBT screws varies significantly according to sex and vertebral body segments, particularly noting the specificity of screw placement at L5. The optimal screw placement strategy should be selected based on the patient's sex and segment characteristics before surgery to maximize the safety and accuracy of CBT screw placement.
期刊介绍:
Orthopaedic Surgery (OS) is the official journal of the Chinese Orthopaedic Association, focusing on all aspects of orthopaedic technique and surgery.
The journal publishes peer-reviewed articles in the following categories: Original Articles, Clinical Articles, Review Articles, Guidelines, Editorials, Commentaries, Surgical Techniques, Case Reports and Meeting Reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


