Karin Nentwich, Karin Klingel, Elena Ene, Julian Müller, Arthur Berkowitz, Sebastian Barth, Thomas Deneke
{"title":"Cardiac sarcoidosis in patients with recurrent ventricular arrhythmias refractory to endocardial ablation.","authors":"Karin Nentwich, Karin Klingel, Elena Ene, Julian Müller, Arthur Berkowitz, Sebastian Barth, Thomas Deneke","doi":"10.1007/s00392-024-02509-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The clinical presentation of cardiac sarcoidosis is diverse. Detection of granuloma in histopathological evaluation proves the diagnosis, but endomyocardial biopsy (EMB) is associated with a high sampling error. However, prompt immunosuppressive therapy may significantly affect patient's prognosis. By analyzing our single center cohort of patients with recurrent ventricular arrhythmias (VA) and nonischemic cardiomyopathy after failure of endocardial ablation, we looked for additional markers supporting the diagnosis of cardiac sarcoidosis.</p><p><strong>Method: </strong>In the last 4 years, 135 patients (mean age 49 y, 63% male) were hospitalized for epicardial ventricular arrhythmia (VA) ablation after failure of endocardial ablation. Nineteen patients had either previously received a diagnosis of cardiac sarcoidosis or were newly diagnosed. The mean follow-up time was 4.3 years. The ECG criteria, primary manifestation, histological findings in EMB, history of VT ablation, distribution of scars on MRI, electroanatomical mapping (EAM), PET CT findings, presence of atrial tachycardias, valve disease and comorbidities were analyzed.</p><p><strong>Results: </strong>Six of 19 (32%) patients showed right bundle block; 6 of 19 (32%) had AV nodal disease, including 4 patients with AV-block III; and 14 patients (73%) primarily presented with ventricular arrhythmias (including 3 with cardiac arrest). In all 19 patients cardiac EMB revealed elevated CD68 macrophages and CD3 T lymphocytes, and 7 of 19 were positive for granuloma (36,8%). Six of 6 patients (100%) undergoing PET CT showed acute inflammation. By analyzing the scar distribution, the most common locations were basal anteroseptal, basal inferoseptal, mid inferoseptal, mid inferior and the septal RV/RVOT. (septal substrate in 100%). There was a high correlation between the findings on the MRIs and low voltage in the electroanatomical mapping EAM). All patients received an immunosuppressive therapy. No patient died during follow-up, 1 patient had a high urgent heart transplant after withdrawal of steroid therapy.</p><p><strong>Conclusion: </strong>Chronic untreated inflammation may be the underlying pathophysiology for patients with unspecific cardiomyopathy and recurrent VA refractory to endocardial and epicardial ablation. Septal substrate in the EAM/MRI, elevated CD3 lymphocytes in the EBM and inflammation in the PET CT may indicate the possible diagnosis of cardiac sarcoidosis. Initializing immunosuppressive therapy in patients with this dedicated constellation with should be taken into consideration.</p>","PeriodicalId":10474,"journal":{"name":"Clinical Research in Cardiology","volume":" ","pages":"1176-1184"},"PeriodicalIF":3.7000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Research in Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00392-024-02509-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The clinical presentation of cardiac sarcoidosis is diverse. Detection of granuloma in histopathological evaluation proves the diagnosis, but endomyocardial biopsy (EMB) is associated with a high sampling error. However, prompt immunosuppressive therapy may significantly affect patient's prognosis. By analyzing our single center cohort of patients with recurrent ventricular arrhythmias (VA) and nonischemic cardiomyopathy after failure of endocardial ablation, we looked for additional markers supporting the diagnosis of cardiac sarcoidosis.
Method: In the last 4 years, 135 patients (mean age 49 y, 63% male) were hospitalized for epicardial ventricular arrhythmia (VA) ablation after failure of endocardial ablation. Nineteen patients had either previously received a diagnosis of cardiac sarcoidosis or were newly diagnosed. The mean follow-up time was 4.3 years. The ECG criteria, primary manifestation, histological findings in EMB, history of VT ablation, distribution of scars on MRI, electroanatomical mapping (EAM), PET CT findings, presence of atrial tachycardias, valve disease and comorbidities were analyzed.
Results: Six of 19 (32%) patients showed right bundle block; 6 of 19 (32%) had AV nodal disease, including 4 patients with AV-block III; and 14 patients (73%) primarily presented with ventricular arrhythmias (including 3 with cardiac arrest). In all 19 patients cardiac EMB revealed elevated CD68 macrophages and CD3 T lymphocytes, and 7 of 19 were positive for granuloma (36,8%). Six of 6 patients (100%) undergoing PET CT showed acute inflammation. By analyzing the scar distribution, the most common locations were basal anteroseptal, basal inferoseptal, mid inferoseptal, mid inferior and the septal RV/RVOT. (septal substrate in 100%). There was a high correlation between the findings on the MRIs and low voltage in the electroanatomical mapping EAM). All patients received an immunosuppressive therapy. No patient died during follow-up, 1 patient had a high urgent heart transplant after withdrawal of steroid therapy.
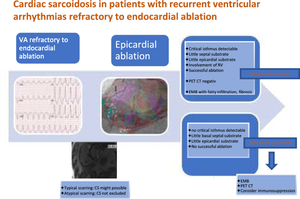
Conclusion: Chronic untreated inflammation may be the underlying pathophysiology for patients with unspecific cardiomyopathy and recurrent VA refractory to endocardial and epicardial ablation. Septal substrate in the EAM/MRI, elevated CD3 lymphocytes in the EBM and inflammation in the PET CT may indicate the possible diagnosis of cardiac sarcoidosis. Initializing immunosuppressive therapy in patients with this dedicated constellation with should be taken into consideration.
期刊介绍:
Clinical Research in Cardiology is an international journal for clinical cardiovascular research. It provides a forum for original and review articles as well as critical perspective articles. Articles are only accepted if they meet stringent scientific standards and have undergone peer review. The journal regularly receives articles from the field of clinical cardiology, angiology, as well as heart and vascular surgery.
As the official journal of the German Cardiac Society, it gives a current and competent survey on the diagnosis and therapy of heart and vascular diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


