Michael C Blayney, Matthew J Reed, John A Masterson, Atul Anand, Matt M Bouamrane, Jacques Fleuriot, Saturnino Luz, Marcus J Lyall, Stewart Mercer, Nicholas L Mills, Susan D Shenkin, Timothy S Walsh, Sarah H Wild, Honghan Wu, Stela McLachlan, Bruce Guthrie, Nazir I Lone
{"title":"Multimorbidity and adverse outcomes following emergency department attendance: population based cohort study.","authors":"Michael C Blayney, Matthew J Reed, John A Masterson, Atul Anand, Matt M Bouamrane, Jacques Fleuriot, Saturnino Luz, Marcus J Lyall, Stewart Mercer, Nicholas L Mills, Susan D Shenkin, Timothy S Walsh, Sarah H Wild, Honghan Wu, Stela McLachlan, Bruce Guthrie, Nazir I Lone","doi":"10.1136/bmjmed-2023-000731","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong></p><p><strong>Objectives: </strong>To describe the effect of multimorbidity on adverse patient centred outcomes in people attending emergency department.</p><p><strong>Design: </strong>Population based cohort study.</p><p><strong>Setting: </strong>Emergency departments in NHS Lothian in Scotland, from 1 January 2012 to 31 December 2019.</p><p><strong>Participants: </strong>Adults (≥18 years) attending emergency departments.</p><p><strong>Data sources: </strong>Linked data from emergency departments, hospital discharges, and cancer registries, and national mortality data.</p><p><strong>Main outcome measures: </strong>Multimorbidity was defined as at least two conditions from the Elixhauser comorbidity index. Multivariable logistic or linear regression was used to assess associations of multimorbidity with 30 day mortality (primary outcome), hospital admission, reattendance at the emergency department within seven days, and time spent in emergency department (secondary outcomes). Primary analysis was stratified by age (<65 <i>v</i> ≥65 years).</p><p><strong>Results: </strong>451 291 people had 1 273 937 attendances to emergency departments during the study period. 43 504 (9.6%) had multimorbidity, and people with multimorbidity were older (median 73 <i>v</i> 43 years), more likely to arrive by emergency ambulance (57.8% <i>v</i> 23.7%), and more likely to be triaged as very urgent (23.5% <i>v</i> 9.2%) than people who do not have multimorbidity. After adjusting for other prognostic covariates, multimorbidity, compared with no multimorbidity, was associated with higher 30 day mortality (8.2% <i>v</i> 1.2%, adjusted odds ratio 1.81 (95% confidence interval (CI) 1.72 to 1.91)), higher rate of hospital admission (60.1% <i>v</i> 20.5%, 1.81 (1.76 to 1.86)), higher reattendance to an emergency department within seven days (7.8% <i>v</i> 3.5%, 1.41 (1.32 to 1.50)), and longer time spent in the department (adjusted coefficient 0.27 h (95% CI 0.26 to 0.27)). The size of associations between multimorbidity and all outcomes were larger in younger patients: for example, the adjusted odds ratio of 30 day mortality was 3.03 (95% CI 2.68 to 3.42) in people younger than 65 years versus 1.61 (95% CI 1.53 to 1.71) in those 65 years or older.</p><p><strong>Conclusions: </strong>Almost one in ten patients presenting to emergency department had multimorbidity using Elixhauser index conditions. Multimorbidity was strongly associated with adverse outcomes and these associations were stronger in younger people. The increasing prevalence of multimorbidity in the population is likely to exacerbate strain on emergency departments unless practice and policy evolve to meet the growing demand.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"3 1","pages":"e000731"},"PeriodicalIF":10.0000,"publicationDate":"2024-08-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11344864/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2023-000731","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Abstract:
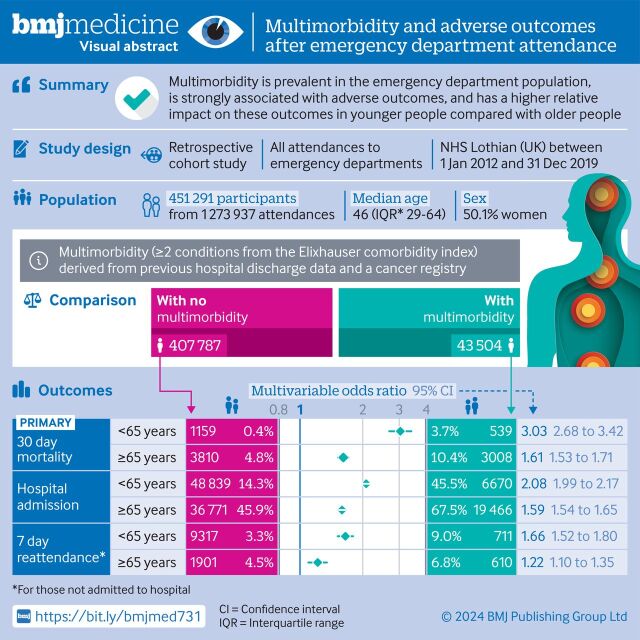
Objectives: To describe the effect of multimorbidity on adverse patient centred outcomes in people attending emergency department.
Design: Population based cohort study.
Setting: Emergency departments in NHS Lothian in Scotland, from 1 January 2012 to 31 December 2019.
Data sources: Linked data from emergency departments, hospital discharges, and cancer registries, and national mortality data.
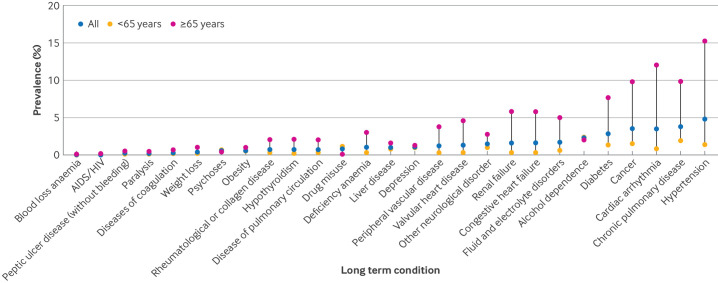
Main outcome measures: Multimorbidity was defined as at least two conditions from the Elixhauser comorbidity index. Multivariable logistic or linear regression was used to assess associations of multimorbidity with 30 day mortality (primary outcome), hospital admission, reattendance at the emergency department within seven days, and time spent in emergency department (secondary outcomes). Primary analysis was stratified by age (<65 v ≥65 years).
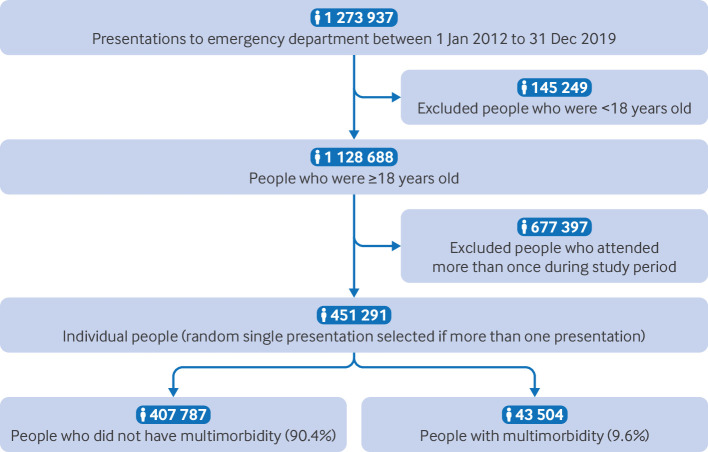
Results: 451 291 people had 1 273 937 attendances to emergency departments during the study period. 43 504 (9.6%) had multimorbidity, and people with multimorbidity were older (median 73 v 43 years), more likely to arrive by emergency ambulance (57.8% v 23.7%), and more likely to be triaged as very urgent (23.5% v 9.2%) than people who do not have multimorbidity. After adjusting for other prognostic covariates, multimorbidity, compared with no multimorbidity, was associated with higher 30 day mortality (8.2% v 1.2%, adjusted odds ratio 1.81 (95% confidence interval (CI) 1.72 to 1.91)), higher rate of hospital admission (60.1% v 20.5%, 1.81 (1.76 to 1.86)), higher reattendance to an emergency department within seven days (7.8% v 3.5%, 1.41 (1.32 to 1.50)), and longer time spent in the department (adjusted coefficient 0.27 h (95% CI 0.26 to 0.27)). The size of associations between multimorbidity and all outcomes were larger in younger patients: for example, the adjusted odds ratio of 30 day mortality was 3.03 (95% CI 2.68 to 3.42) in people younger than 65 years versus 1.61 (95% CI 1.53 to 1.71) in those 65 years or older.
Conclusions: Almost one in ten patients presenting to emergency department had multimorbidity using Elixhauser index conditions. Multimorbidity was strongly associated with adverse outcomes and these associations were stronger in younger people. The increasing prevalence of multimorbidity in the population is likely to exacerbate strain on emergency departments unless practice and policy evolve to meet the growing demand.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


