Zhe Xu, Juliet Usher-Smith, Lisa Pennells, Ryan Chung, Matthew Arnold, Lois Kim, Stephen Kaptoge, Matthew Sperrin, Emanuele Di Angelantonio, Angela M Wood
{"title":"Age and sex specific thresholds for risk stratification of cardiovascular disease and clinical decision making: prospective open cohort study.","authors":"Zhe Xu, Juliet Usher-Smith, Lisa Pennells, Ryan Chung, Matthew Arnold, Lois Kim, Stephen Kaptoge, Matthew Sperrin, Emanuele Di Angelantonio, Angela M Wood","doi":"10.1136/bmjmed-2023-000633","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To quantify the potential advantages of using 10 year risk prediction models for cardiovascular disease, in combination with risk thresholds specific to both age and sex, to identify individuals at high risk of cardiovascular disease for allocation of statin treatment.</p><p><strong>Design: </strong>Prospective open cohort study.</p><p><strong>Setting: </strong>Primary care data from the UK Clinical Practice Research Datalink GOLD, linked with hospital admissions from Hospital Episode Statistics and national mortality records from the Office for National Statistics in England, 1 January 2006 to 31 May 2019.</p><p><strong>Participants: </strong>1 046 736 individuals (aged 40-85 years) with no cardiovascular disease, diabetes, or a history of statin treatment at baseline using data from electronic health records.</p><p><strong>Main outcome measures: </strong>10 year risk of cardiovascular disease, calculated with version 2 of the QRISK cardiovascular disease risk algorithm (QRISK2), with two main strategies to identify individuals at high risk: in strategy A, estimated risk was a fixed cut-off value of ≥10% (ie, as per the UK National Institute for Health and Care Excellence guidelines); in strategy B, estimated risk was ≥10% or ≥90th centile of age and sex specific risk distributions.</p><p><strong>Results: </strong>Compared with strategy A, strategy B stratified 20 241 (149.8%) more women aged ≤53 years and 9832 (150.2%) more men aged ≤47 years as having a high risk of cardiovascular disease; for all other ages the strategies were the same. Assuming that treatment with statins would be initiated in those identified as high risk, differences in the estimated gain in cardiovascular disease-free life years from statin treatment for strategy B versus strategy A were 0.14 and 0.16 years for women and men aged 40 years, respectively; among individuals aged 40-49 years, the numbers needed to treat to prevent one cardiovascular disease event for strategy B versus strategy A were 39 versus 21 in women and 19 versus 15 in men, respectively.</p><p><strong>Conclusions: </strong>This study quantified the potential gains in cardiovascular disease-free life years when implementing prevention strategies based on age and sex specific risk thresholds instead of a fixed risk threshold for allocation of statin treatment. Such gains should be weighed against the costs of treating more younger people with statins for longer.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"3 1","pages":"e000633"},"PeriodicalIF":10.0000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11340247/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2023-000633","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To quantify the potential advantages of using 10 year risk prediction models for cardiovascular disease, in combination with risk thresholds specific to both age and sex, to identify individuals at high risk of cardiovascular disease for allocation of statin treatment.
Design: Prospective open cohort study.
Setting: Primary care data from the UK Clinical Practice Research Datalink GOLD, linked with hospital admissions from Hospital Episode Statistics and national mortality records from the Office for National Statistics in England, 1 January 2006 to 31 May 2019.
Participants: 1 046 736 individuals (aged 40-85 years) with no cardiovascular disease, diabetes, or a history of statin treatment at baseline using data from electronic health records.
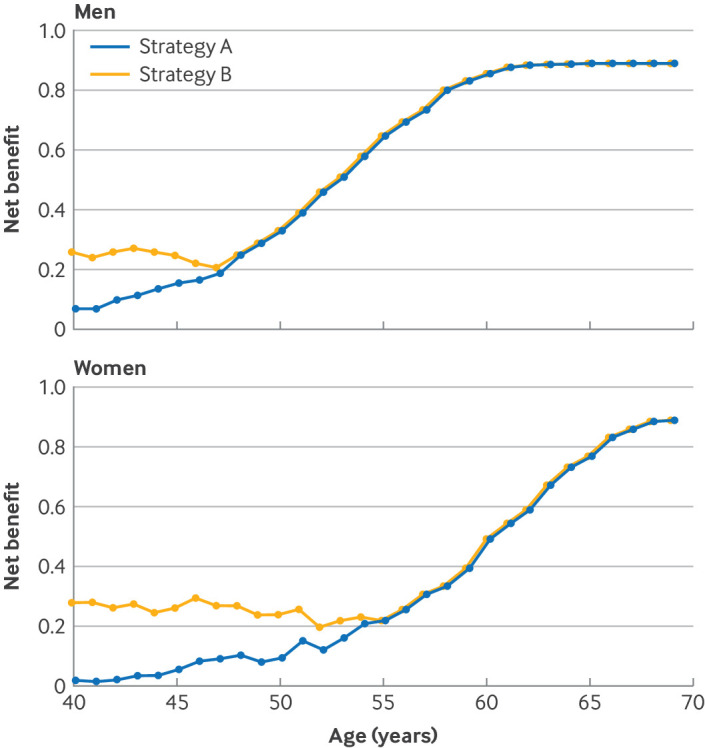
Main outcome measures: 10 year risk of cardiovascular disease, calculated with version 2 of the QRISK cardiovascular disease risk algorithm (QRISK2), with two main strategies to identify individuals at high risk: in strategy A, estimated risk was a fixed cut-off value of ≥10% (ie, as per the UK National Institute for Health and Care Excellence guidelines); in strategy B, estimated risk was ≥10% or ≥90th centile of age and sex specific risk distributions.
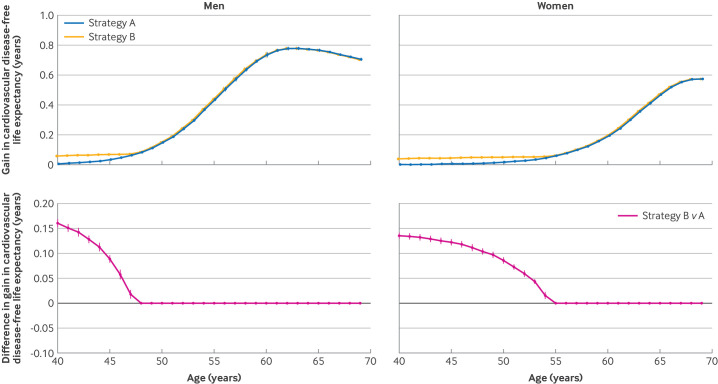
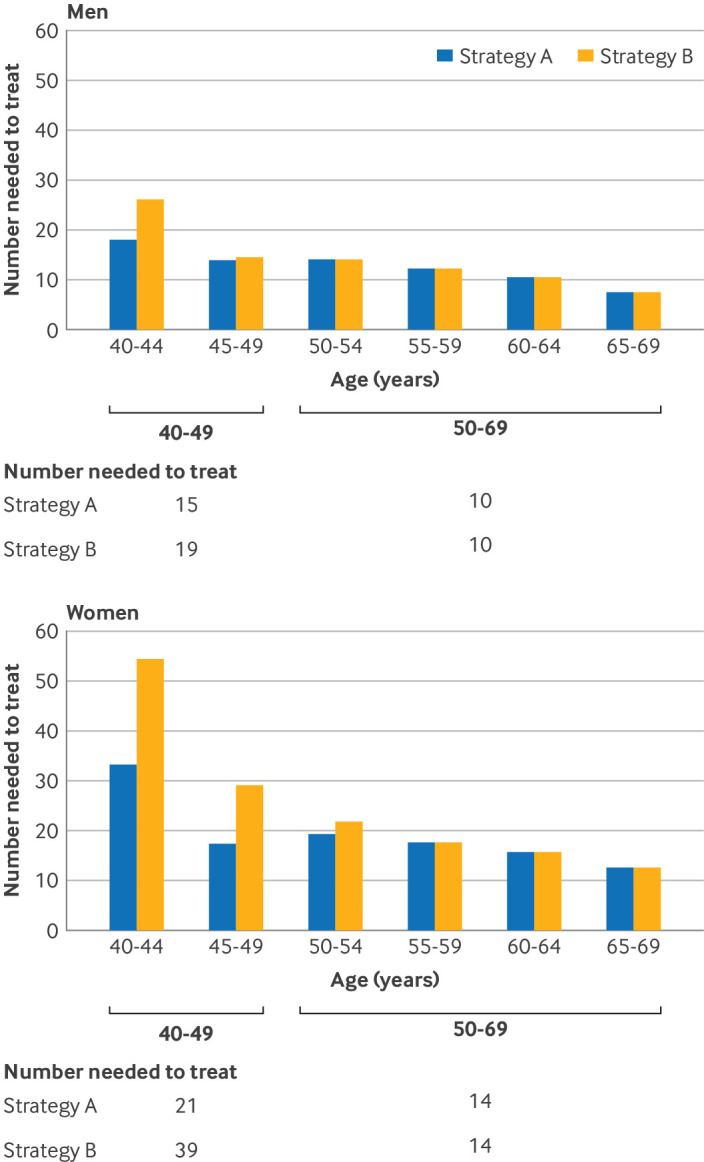
Results: Compared with strategy A, strategy B stratified 20 241 (149.8%) more women aged ≤53 years and 9832 (150.2%) more men aged ≤47 years as having a high risk of cardiovascular disease; for all other ages the strategies were the same. Assuming that treatment with statins would be initiated in those identified as high risk, differences in the estimated gain in cardiovascular disease-free life years from statin treatment for strategy B versus strategy A were 0.14 and 0.16 years for women and men aged 40 years, respectively; among individuals aged 40-49 years, the numbers needed to treat to prevent one cardiovascular disease event for strategy B versus strategy A were 39 versus 21 in women and 19 versus 15 in men, respectively.
Conclusions: This study quantified the potential gains in cardiovascular disease-free life years when implementing prevention strategies based on age and sex specific risk thresholds instead of a fixed risk threshold for allocation of statin treatment. Such gains should be weighed against the costs of treating more younger people with statins for longer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


