Brittany Park, Zena Alani, Edrick Sulistio, Ahmed W H Barazanchi, Jonathan Koea, Alain Vandal, Andrew G Hill, Andrew D MacCormick
{"title":"Frailty using the Clinical Frailty Scale to predict short- and long-term adverse outcomes following emergency laparotomy: meta-analysis.","authors":"Brittany Park, Zena Alani, Edrick Sulistio, Ahmed W H Barazanchi, Jonathan Koea, Alain Vandal, Andrew G Hill, Andrew D MacCormick","doi":"10.1093/bjsopen/zrae078","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Emergency laparotomy has high morbidity and mortality rates. Frailty assessment remains underutilized in this setting, in part due to time constraints and feasibility. The Clinical Frailty Scale has been identified as the most appropriate tool for frailty assessment in emergency laparotomy patients and is recommended for all older patients undergoing emergency laparotomy. The prognostic impact of measured frailty using the Clinical Frailty Scale on short- and long-term mortality and morbidity rates remains to be determined.</p><p><strong>Methods: </strong>Observational cohort studies were identified by systematically searching Medline, Embase, Scopus and CENTRAL databases up to February 2024, comparing outcomes following emergency laparotomy for frail and non-frail participants defined according to the Clinical Frailty Scale. The primary outcomes were short- and long-term mortality rates. A random-effects model was created with pooling of effect estimates and a separate narrative synthesis was created. Risk of bias was assessed.</p><p><strong>Results: </strong>Twelve articles comprising 5704 patients were included. Frailty prevalence was 25% in all patients and 32% in older adults (age ≥55 years). Older patients with frailty had a significantly greater risk of postoperative death (30-day mortality rate OR 3.84, 95% c.i. 2.90 to 5.09, 1-year mortality rate OR 3.03, 95% c.i. 2.17 to 4.23). Meta-regression revealed that variations in cut-off values to define frailty did not significantly affect the association with frailty and 30-day mortality rate. Frailty was associated with higher rates of major complications (OR 1.93, 95% c.i. 1.27 to 2.93) and discharge to an increased level of care.</p><p><strong>Conclusion: </strong>Frailty is significantly correlated with short- and long-term mortality rates following emergency laparotomy, as well as an adverse morbidity rate and functional outcomes. Identifying frailty using the Clinical Frailty Scale may aid in patient-centred decision-making and implementation of tailored care strategies for these 'high-risk' patients, with the aim of reducing adverse outcomes following emergency laparotomy.</p>","PeriodicalId":9028,"journal":{"name":"BJS Open","volume":"8 4","pages":""},"PeriodicalIF":4.5000,"publicationDate":"2024-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11336663/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJS Open","FirstCategoryId":"88","ListUrlMain":"https://doi.org/10.1093/bjsopen/zrae078","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Emergency laparotomy has high morbidity and mortality rates. Frailty assessment remains underutilized in this setting, in part due to time constraints and feasibility. The Clinical Frailty Scale has been identified as the most appropriate tool for frailty assessment in emergency laparotomy patients and is recommended for all older patients undergoing emergency laparotomy. The prognostic impact of measured frailty using the Clinical Frailty Scale on short- and long-term mortality and morbidity rates remains to be determined.
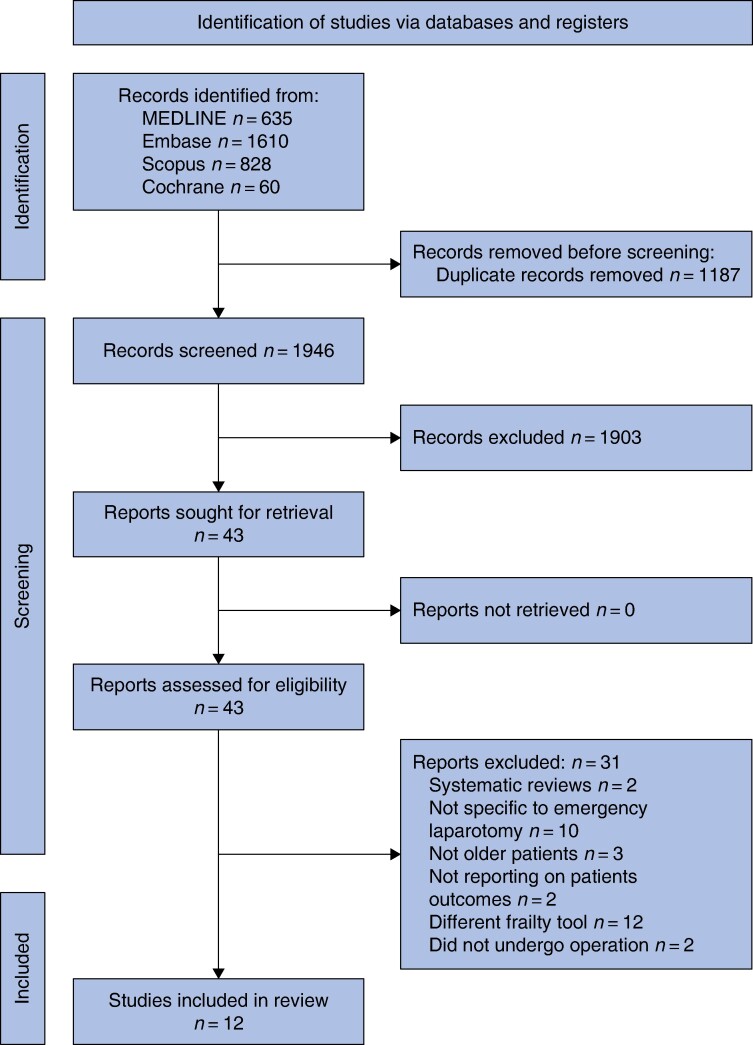
Methods: Observational cohort studies were identified by systematically searching Medline, Embase, Scopus and CENTRAL databases up to February 2024, comparing outcomes following emergency laparotomy for frail and non-frail participants defined according to the Clinical Frailty Scale. The primary outcomes were short- and long-term mortality rates. A random-effects model was created with pooling of effect estimates and a separate narrative synthesis was created. Risk of bias was assessed.
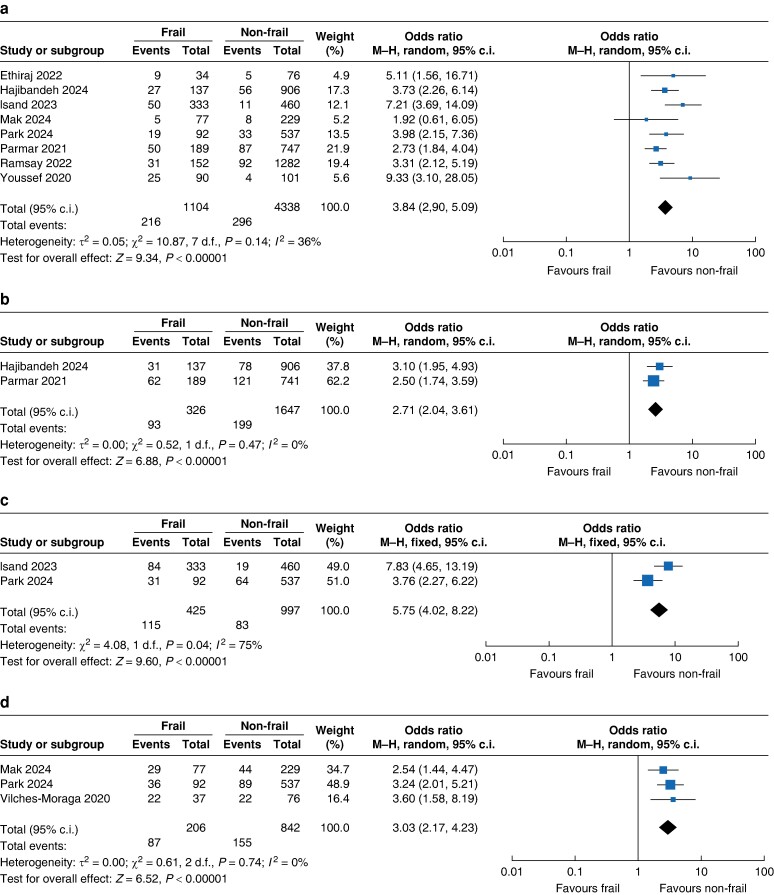
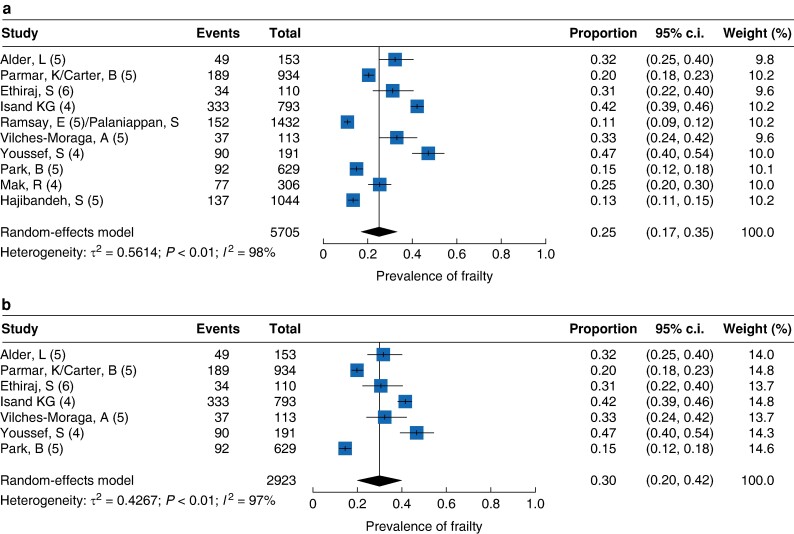
Results: Twelve articles comprising 5704 patients were included. Frailty prevalence was 25% in all patients and 32% in older adults (age ≥55 years). Older patients with frailty had a significantly greater risk of postoperative death (30-day mortality rate OR 3.84, 95% c.i. 2.90 to 5.09, 1-year mortality rate OR 3.03, 95% c.i. 2.17 to 4.23). Meta-regression revealed that variations in cut-off values to define frailty did not significantly affect the association with frailty and 30-day mortality rate. Frailty was associated with higher rates of major complications (OR 1.93, 95% c.i. 1.27 to 2.93) and discharge to an increased level of care.
Conclusion: Frailty is significantly correlated with short- and long-term mortality rates following emergency laparotomy, as well as an adverse morbidity rate and functional outcomes. Identifying frailty using the Clinical Frailty Scale may aid in patient-centred decision-making and implementation of tailored care strategies for these 'high-risk' patients, with the aim of reducing adverse outcomes following emergency laparotomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


