Marcus Westerberg , Hans Garmo , David Robinson , Pär Stattin , Rolf Gedeborg
{"title":"Target trial emulation using new comorbidity indices provided risk estimates comparable to a randomized trial","authors":"Marcus Westerberg , Hans Garmo , David Robinson , Pär Stattin , Rolf Gedeborg","doi":"10.1016/j.jclinepi.2024.111504","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><p>To quantify the ability of two new comorbidity indices to adjust for confounding, by benchmarking a target trial emulation against the randomized controlled trial (RCT) result.</p></div><div><h3>Study Design and Setting</h3><p>Observational study including 18,316 men from Prostate Cancer data Base Sweden 5.0, diagnosed with prostate cancer between 2008 and 2019 and treated with primary radical prostatectomy (RP, <em>n</em> = 14,379) or radiotherapy (RT, <em>n</em> = 3,937). The effect on adjusted risk of death from any cause after adjustment for comorbidity by use of two new comorbidity indices, the multidimensional diagnosis-based comorbidity index and the drug comorbidity index, were compared to adjustment for the Charlson comorbidity index (CCI).</p></div><div><h3>Results</h3><p>Risk of death was higher after RT than RP (hazard ratio [HR] = 1.94; 95% confidence interval [CI]: 1.70–2.21). The difference decreased when adjusting for age, cancer characteristics, and CCI (HR = 1.32, 95% CI: 1.06–1.66). Adjustment for the two new comorbidity indices further attenuated the difference (HR 1.14, 95% CI 0.91–1.44). Emulation of a hypothetical pragmatic trial where also older men with any type of baseline comorbidity were included, largely confirmed these results (HR 1.10; 95% CI 0.95–1.26).</p></div><div><h3>Conclusion</h3><p>Adjustment for comorbidity using two new indices provided comparable risk of death from any cause in line with results of a RCT. Similar results were seen in a broader study population, more representative of clinical practice.</p></div>","PeriodicalId":51079,"journal":{"name":"Journal of Clinical Epidemiology","volume":"174 ","pages":"Article 111504"},"PeriodicalIF":7.3000,"publicationDate":"2024-08-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0895435624002609/pdfft?md5=66bdbf3013b9d88ca0da75aec3fcdb62&pid=1-s2.0-S0895435624002609-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0895435624002609","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives
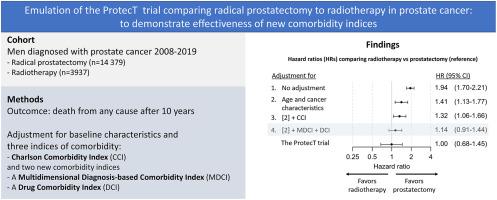
To quantify the ability of two new comorbidity indices to adjust for confounding, by benchmarking a target trial emulation against the randomized controlled trial (RCT) result.
Study Design and Setting
Observational study including 18,316 men from Prostate Cancer data Base Sweden 5.0, diagnosed with prostate cancer between 2008 and 2019 and treated with primary radical prostatectomy (RP, n = 14,379) or radiotherapy (RT, n = 3,937). The effect on adjusted risk of death from any cause after adjustment for comorbidity by use of two new comorbidity indices, the multidimensional diagnosis-based comorbidity index and the drug comorbidity index, were compared to adjustment for the Charlson comorbidity index (CCI).
Results
Risk of death was higher after RT than RP (hazard ratio [HR] = 1.94; 95% confidence interval [CI]: 1.70–2.21). The difference decreased when adjusting for age, cancer characteristics, and CCI (HR = 1.32, 95% CI: 1.06–1.66). Adjustment for the two new comorbidity indices further attenuated the difference (HR 1.14, 95% CI 0.91–1.44). Emulation of a hypothetical pragmatic trial where also older men with any type of baseline comorbidity were included, largely confirmed these results (HR 1.10; 95% CI 0.95–1.26).
Conclusion
Adjustment for comorbidity using two new indices provided comparable risk of death from any cause in line with results of a RCT. Similar results were seen in a broader study population, more representative of clinical practice.
期刊介绍:
The Journal of Clinical Epidemiology strives to enhance the quality of clinical and patient-oriented healthcare research by advancing and applying innovative methods in conducting, presenting, synthesizing, disseminating, and translating research results into optimal clinical practice. Special emphasis is placed on training new generations of scientists and clinical practice leaders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


