{"title":"Predictors of fluid overload in allogeneic hematopoietic cell transplant patients receiving post-transplant cyclophosphamide.","authors":"Megan Tsao, Rasmus Hoeg, Joshua Pecoraro, Megan Kuehner, Brittany Deen, Julie Guglielmo","doi":"10.1177/10781552241276418","DOIUrl":null,"url":null,"abstract":"<p><p>BackgroundFluid overload (FO) commonly occurs during hospitalization for allogeneic hematopoietic cell transplantation (HCT). Grade 2-4 FO is associated with day +100 non-relapse mortality.1 Post-transplant cyclophosphamide (PTCY) for graft-versus-host disease prevention requires aggressive IV hydration to prevent hemorrhagic cystitis.Materials and MethodsThis is a single-center, retrospective, observational study conducted at an academic medical center via electronic chart review. Included patients received allogeneic HCT followed by PTCY on days +3 and +4. Patients were excluded for age < 18 years or incarceration. Primary endpoints are incidence of Grade 2-4 FO and associated risk factors. Descriptive and inferential statistics (i.e., <b>Fisher's exact test</b>, <b>multivariable regression analysis) were</b> used.ResultsOf 97 patients screened, 95 were included and 2 were excluded due to absence of weight measurements needed to grade FO. Median age was 60 years, 66.3% were male, 91.6% received reduced-intensity conditioning, 72.6% received haploidentical HCT, 44.2% were ECOG 0, and 11.6% had diastolic dysfunction. Incidence of grade 2-4 FO was 33.7% (n = 32). Univariate analyses found age (continuous; p = 0.04) and BSA < 1.7 m<sup>2</sup> (p = 0.006) as independent factors associated with grade 2-4 FO. Multivariable regression analysis found 3.3% higher risk with every 1-year increase in age ranging from f 20 to 78 years (OR 1.033, 95% CI 1.001, 1.006; p = 0.0453) and 82.8% lower risk with BSA ≥ 1.7 m<sup>2</sup> (OR 0.172, 95% CI 0.051, 0.588; p = 0.005) after adjusting for co-variates.Conclusion(s)Increasing age and BSA < 1.7 m<sup>2</sup> are risk factors associated with grade 2-4 FO during hospitalization for allogeneic HCT with PTCY.</p>","PeriodicalId":16637,"journal":{"name":"Journal of Oncology Pharmacy Practice","volume":" ","pages":"1046-1050"},"PeriodicalIF":0.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12426334/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Oncology Pharmacy Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/10781552241276418","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/18 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
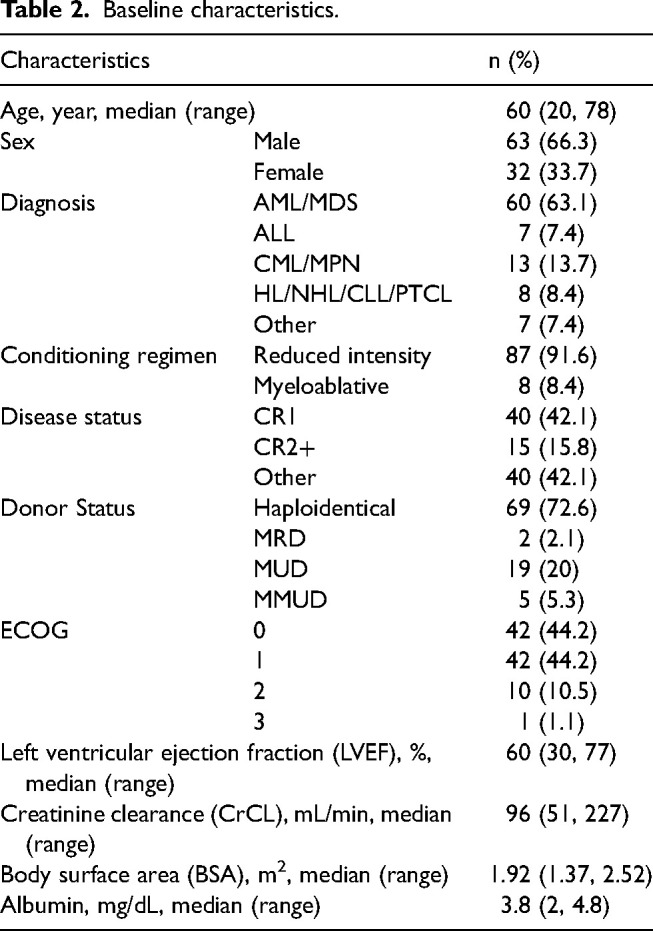
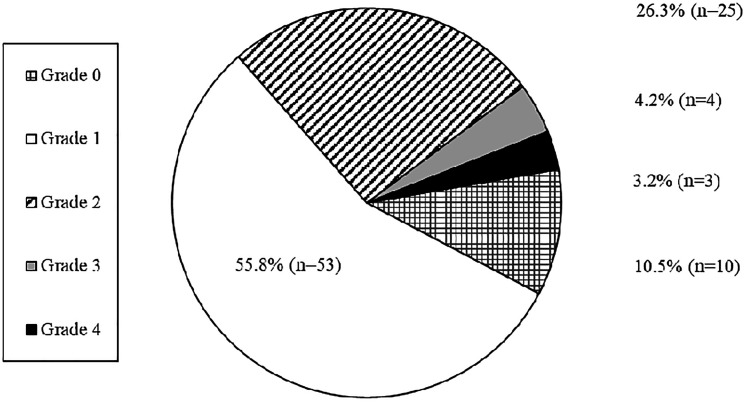
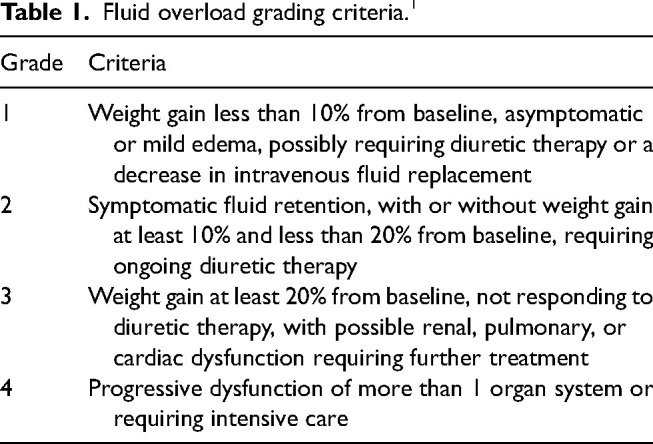
BackgroundFluid overload (FO) commonly occurs during hospitalization for allogeneic hematopoietic cell transplantation (HCT). Grade 2-4 FO is associated with day +100 non-relapse mortality.1 Post-transplant cyclophosphamide (PTCY) for graft-versus-host disease prevention requires aggressive IV hydration to prevent hemorrhagic cystitis.Materials and MethodsThis is a single-center, retrospective, observational study conducted at an academic medical center via electronic chart review. Included patients received allogeneic HCT followed by PTCY on days +3 and +4. Patients were excluded for age < 18 years or incarceration. Primary endpoints are incidence of Grade 2-4 FO and associated risk factors. Descriptive and inferential statistics (i.e., Fisher's exact test, multivariable regression analysis) were used.ResultsOf 97 patients screened, 95 were included and 2 were excluded due to absence of weight measurements needed to grade FO. Median age was 60 years, 66.3% were male, 91.6% received reduced-intensity conditioning, 72.6% received haploidentical HCT, 44.2% were ECOG 0, and 11.6% had diastolic dysfunction. Incidence of grade 2-4 FO was 33.7% (n = 32). Univariate analyses found age (continuous; p = 0.04) and BSA < 1.7 m2 (p = 0.006) as independent factors associated with grade 2-4 FO. Multivariable regression analysis found 3.3% higher risk with every 1-year increase in age ranging from f 20 to 78 years (OR 1.033, 95% CI 1.001, 1.006; p = 0.0453) and 82.8% lower risk with BSA ≥ 1.7 m2 (OR 0.172, 95% CI 0.051, 0.588; p = 0.005) after adjusting for co-variates.Conclusion(s)Increasing age and BSA < 1.7 m2 are risk factors associated with grade 2-4 FO during hospitalization for allogeneic HCT with PTCY.
期刊介绍:
Journal of Oncology Pharmacy Practice is a peer-reviewed scholarly journal dedicated to educating health professionals about providing pharmaceutical care to patients with cancer. It is the official publication of the International Society for Oncology Pharmacy Practitioners (ISOPP). Publishing pertinent case reports and consensus guidelines...

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


