Analysis of Determinants of Stunting and Identifications of Stunting Risk Profiles Among Under 2-Year-Old Children in Ethiopia. A Latent Class Analysis.
{"title":"Analysis of Determinants of Stunting and Identifications of Stunting Risk Profiles Among Under 2-Year-Old Children in Ethiopia. A Latent Class Analysis.","authors":"Anteneh Fikrie, Berhanu Adula, Jitu Beka, Dejene Hailu, Cheru Atsmegiorgis Kitabo, Mark Spigt","doi":"10.1177/23333928241271921","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Childhood stunting has a long-term impact on cognitive development and overall well-being. Understanding varying stunting profiles is crucial for targeted interventions and effective policy-making. Therefore, our study aimed to identify the determinants and stunting risk profiles among 2-year-old children in Ethiopia.</p><p><strong>Methods and materials: </strong>A cross-sectional study was conducted on 395 mother-child pairs attending selected public health centers for growth monitoring and promotion under 5 outpatient departments and immunization services. The data were collected by face-to-face interviews, with the anthropometric data collected using the procedure stipulated by the World Health Organization. The data were entered using Epi Data version 4.6 and exported to STATA 16 and Jamovi version 2.3.28 for analysis. Bayesian logistic regression analysis was conducted to identify potential factors of stunting. Likewise, lifecycle assessment analysis (LCA) was used to examine the heterogeneity of the magnitude of stunting.</p><p><strong>Results: </strong>The overall prevalence of stunting in children under 24 months was 47.34% (95% confidence interval (CI): 42.44-52.29%). The LCA identified 3 distinct risk profiles. The first profile is <b>Class 1</b>, which is labeled as low-risk, comprised 23.8% of the children, and had the lowest prevalence of stunting (23.4%). This group characterized as having a lower risk to stunting. The second profile is <b>Class 2</b>, which is identified as high-risk, comprised 47.1%, and had a high prevalence of stunting (66.7%), indicating a higher susceptibility to stunting compared to Class 1. The third profile is <b>Class 3</b>, which is categorized as mixed-risk and had a moderate stunting prevalence of 35.7%, indicating a complex interplay of factors contributing to stunting.</p><p><strong>Conclusion: </strong>Our study identified 3 distinct risk profiles for stunting in young children. A substantial amount (almost half) is in the high-risk category, where stunting is far more common. The identification of stunting profiles necessitates considering heterogeneity in risk factors in interventions. Healthcare practitioners should screen, provide nutrition counseling, and promote breastfeeding. Policymakers should strengthen social safety nets and support primary education.</p>","PeriodicalId":12951,"journal":{"name":"Health Services Research and Managerial Epidemiology","volume":"11 ","pages":"23333928241271921"},"PeriodicalIF":1.5000,"publicationDate":"2024-08-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11329923/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Research and Managerial Epidemiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23333928241271921","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Childhood stunting has a long-term impact on cognitive development and overall well-being. Understanding varying stunting profiles is crucial for targeted interventions and effective policy-making. Therefore, our study aimed to identify the determinants and stunting risk profiles among 2-year-old children in Ethiopia.
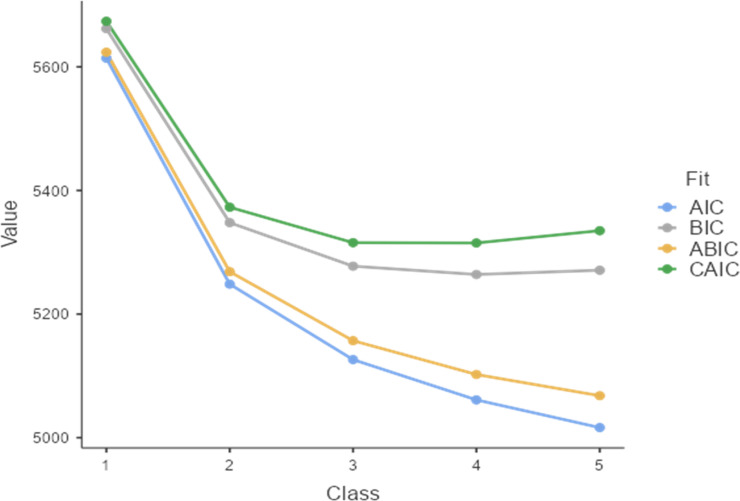
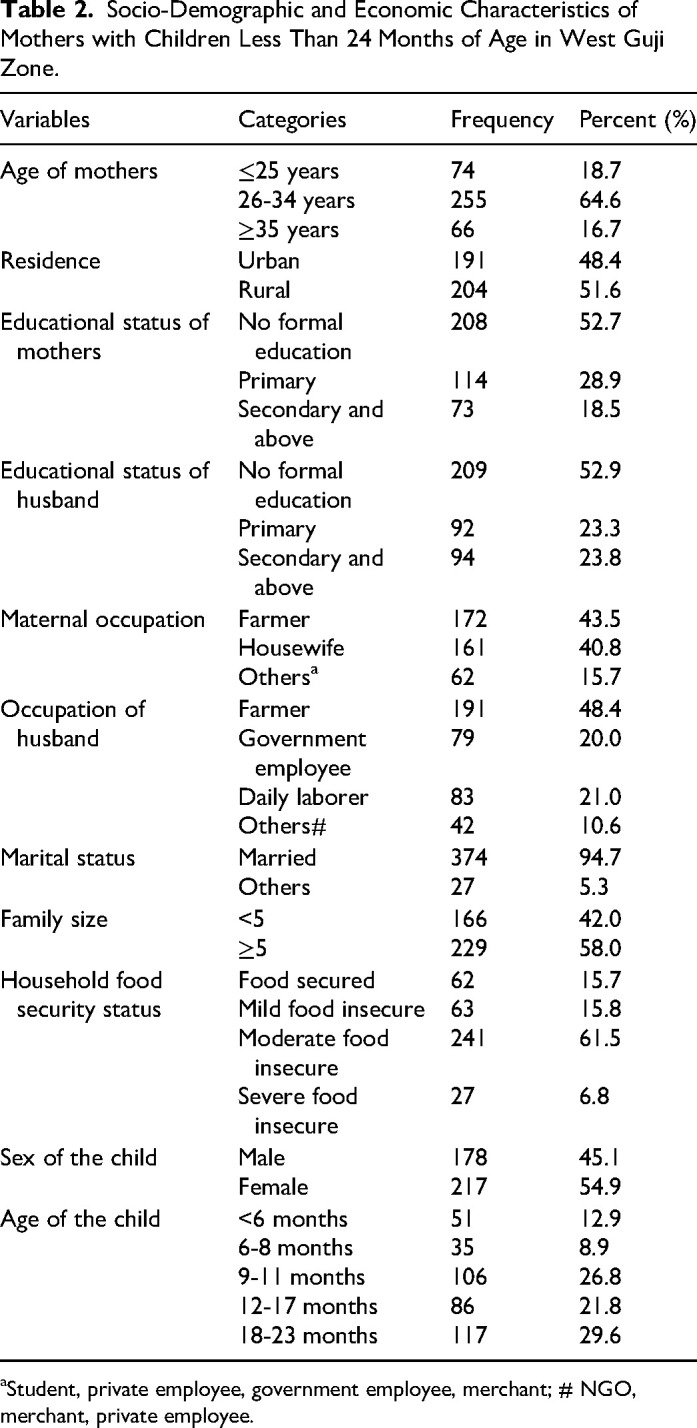
Methods and materials: A cross-sectional study was conducted on 395 mother-child pairs attending selected public health centers for growth monitoring and promotion under 5 outpatient departments and immunization services. The data were collected by face-to-face interviews, with the anthropometric data collected using the procedure stipulated by the World Health Organization. The data were entered using Epi Data version 4.6 and exported to STATA 16 and Jamovi version 2.3.28 for analysis. Bayesian logistic regression analysis was conducted to identify potential factors of stunting. Likewise, lifecycle assessment analysis (LCA) was used to examine the heterogeneity of the magnitude of stunting.
Results: The overall prevalence of stunting in children under 24 months was 47.34% (95% confidence interval (CI): 42.44-52.29%). The LCA identified 3 distinct risk profiles. The first profile is Class 1, which is labeled as low-risk, comprised 23.8% of the children, and had the lowest prevalence of stunting (23.4%). This group characterized as having a lower risk to stunting. The second profile is Class 2, which is identified as high-risk, comprised 47.1%, and had a high prevalence of stunting (66.7%), indicating a higher susceptibility to stunting compared to Class 1. The third profile is Class 3, which is categorized as mixed-risk and had a moderate stunting prevalence of 35.7%, indicating a complex interplay of factors contributing to stunting.
Conclusion: Our study identified 3 distinct risk profiles for stunting in young children. A substantial amount (almost half) is in the high-risk category, where stunting is far more common. The identification of stunting profiles necessitates considering heterogeneity in risk factors in interventions. Healthcare practitioners should screen, provide nutrition counseling, and promote breastfeeding. Policymakers should strengthen social safety nets and support primary education.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


