Avi Sabbag MD, Gisella Amoroso MD, Orr Tomer MD, Giulio Conte MD, PhD, Roy Beinart MD, Eyal Nof MD, Tardu Özkartal MD, Pierre Ollitrault MD, Mikael Laredo MD, Oholi Tovia-Brodie MD, Estelle Gandjbakhch MD, PhD, Michele de Benedictis MD, Rachel M. A. ter Bekke MD, PhD, Anat Milman MD
{"title":"Clinical differences between drug-induced type 1 Brugada pattern and syndrome","authors":"Avi Sabbag MD, Gisella Amoroso MD, Orr Tomer MD, Giulio Conte MD, PhD, Roy Beinart MD, Eyal Nof MD, Tardu Özkartal MD, Pierre Ollitrault MD, Mikael Laredo MD, Oholi Tovia-Brodie MD, Estelle Gandjbakhch MD, PhD, Michele de Benedictis MD, Rachel M. A. ter Bekke MD, PhD, Anat Milman MD","doi":"10.1002/joa3.13053","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Diagnosis of Brugada syndrome (BrS) may be established by exposing a Type 1 Brugada pattern using a sodium channel blocker. Data on the outcomes of different patient populations with drug-induced Type 1 Brugada pattern are limited. The present study reports on the characteristics and outcome of subjects with ajmaline induced Type 1 Brugada pattern.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A multicenter retrospective study including all consecutive cases of ajmaline-induced Type 1 Brugada pattern from seven centers.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 260 patients (69.9% males, mean age 43.4 ± 13.5) were included. Additional characteristics included history of syncope (<i>n</i> = 56, 21.5%), family history of BrS (<i>n</i> = 58, 22.3%) or sudden cardiac death (<i>n</i> = 47, 18.1%) and ventricular fibrillation (<i>n</i> = 3, 1.2%). Patients were divided into those meeting current diagnostic criteria for drug-induced BrS (DIBrS) and compared to the drug-induced Brugada pattern (DIBrECG). Females were significantly overrepresented in the DIBrS group (<i>n</i> = 50, 40% vs. <i>n</i> = 29, 21.5%, <i>p</i> = .001). A significantly higher prevalence of type 2/3 Brugada ECG at baseline was found in the DIBrECG group (<i>n</i> = 108, 80.8% vs. <i>n</i> = 75, 60% in the DIBrS, <i>p</i> = .026). During a median follow up of three (IQR 1.50–5.32) years, a single event of significant arrhythmia occurred in the DIBrS group.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Less than half of subjects with ajmaline-induced Brugada pattern met current criteria for BrS. These individuals had very low rate of adverse outcomes during a follow up of 3 years, irrespective of the indication for the test or eligibility for the BrS diagnosis.</p>\n </section>\n </div>","PeriodicalId":15174,"journal":{"name":"Journal of Arrhythmia","volume":"40 4","pages":"982-990"},"PeriodicalIF":2.2000,"publicationDate":"2024-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11317691/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Arrhythmia","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/joa3.13053","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Diagnosis of Brugada syndrome (BrS) may be established by exposing a Type 1 Brugada pattern using a sodium channel blocker. Data on the outcomes of different patient populations with drug-induced Type 1 Brugada pattern are limited. The present study reports on the characteristics and outcome of subjects with ajmaline induced Type 1 Brugada pattern.
Methods
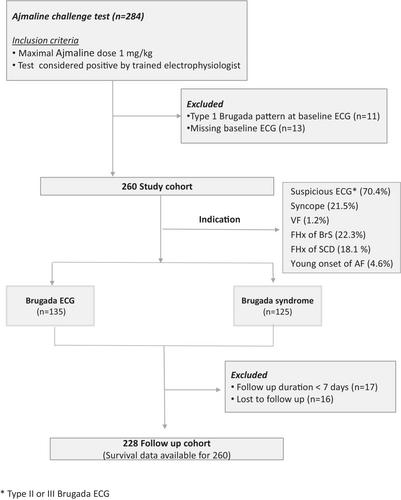
A multicenter retrospective study including all consecutive cases of ajmaline-induced Type 1 Brugada pattern from seven centers.
Results
A total of 260 patients (69.9% males, mean age 43.4 ± 13.5) were included. Additional characteristics included history of syncope (n = 56, 21.5%), family history of BrS (n = 58, 22.3%) or sudden cardiac death (n = 47, 18.1%) and ventricular fibrillation (n = 3, 1.2%). Patients were divided into those meeting current diagnostic criteria for drug-induced BrS (DIBrS) and compared to the drug-induced Brugada pattern (DIBrECG). Females were significantly overrepresented in the DIBrS group (n = 50, 40% vs. n = 29, 21.5%, p = .001). A significantly higher prevalence of type 2/3 Brugada ECG at baseline was found in the DIBrECG group (n = 108, 80.8% vs. n = 75, 60% in the DIBrS, p = .026). During a median follow up of three (IQR 1.50–5.32) years, a single event of significant arrhythmia occurred in the DIBrS group.
Conclusion
Less than half of subjects with ajmaline-induced Brugada pattern met current criteria for BrS. These individuals had very low rate of adverse outcomes during a follow up of 3 years, irrespective of the indication for the test or eligibility for the BrS diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


