Brianna E. Morgan PhD, NP, Harriet Mather MD, Daniel David PhD, RN
{"title":"Surviving aging—An assets-based approach","authors":"Brianna E. Morgan PhD, NP, Harriet Mather MD, Daniel David PhD, RN","doi":"10.1111/jgs.19126","DOIUrl":null,"url":null,"abstract":"<p>Rather than seeking time-bending bodies of water, today's scientists pursue the fountain of youth in older adults who demonstrate younger-than-expected attributes. SuperAgers, for example, exhibit signs of cognitive youth despite advanced age. Researchers seek to extract the fountain of youth from SuperAgers' modifiable risks. A 2020 Lancet Commission report found that addressing 12 modifiable risk factors could potentially prevent 40% of cases of dementia.<span><sup>2</sup></span> While promising, this approach centers around combating aging rather than building upon its inherent assets and opportunities. In this editorial, we discuss the strengths and weaknesses of contemporary conceptual models of aging, highlight an article published in this issue that characterizes factors associated with SuperAgers in a sample of African Americans, and propose a new model of aging (Table 1). We aim to conceptualize an assets-based approach that incorporates both the strengths and challenges faced by all older adults seeking to survive aging.</p><p>SuperAging describes older adults who maintain cognitive function equal to normative middle-aged cohorts and is the guiding framework of the Trammel study. While some heterogeneity exists, SuperAging most frequently characterizes a person who is 80+ years old and performs extremely well on a measure of episodic memory (the Rey Auditory Verbal Learning Task), a single aspect of cognition. SuperAgers resist age-related changes (i.e., display cognitive resilience) and demonstrate neuroanatomical features of adults who are decades younger. The concept of SuperAgers is limited by exclusivity (median—12% of older adults), singular dimension (only episodic memory), and stigmatization for those who fail to meet the criteria.<span><sup>3, 4</sup></span></p><p>Despite rising national awareness of racialized disparities in dementia, cognitive resilience in historically underrepresented racial and ethnic groups remains understudied. Using a nationally representative dataset, Trammel et al. explore differences among 1285 African American participants over 80 years old across three cohorts in the National Alzheimer's Coordinating Center dataset—SuperAgers, cognitively intact, and cognitively impaired. After accounting for gender and educational differences, classification as a SuperAger was associated with reduced prevalence of sleep disorders, decreased depression, and moderate alcohol usage. While SuperAgers exhibited vascular comorbidities comparable to non-SuperAgers, they were more likely to report taking medications, including antihypertensives and nonsteroidal anti-inflammatory drugs. Taken together, the results suggest that 80+-year-old African Americans who actively address chronic health conditions are most likely to demonstrate SuperAging status.</p><p>Research on SuperAgers has been a focus since 2012.<span><sup>5</sup></span> It is quite remarkable that a study investigating SuperAgers in African American cohorts has not been conducted earlier. Applying aging frameworks to groups historically underrepresented in research (e.g., African American SuperAgers) can help to illuminate how well these frameworks integrate the experiences of all older adults. The strength of the SuperAging framework is its specificity. Inclusion is a single concrete measure with a defined threshold. However, while SuperAging reveals the remarkable capacity of older adults, very few will attain this status. A mere 4.7% of the sample in Trammel's cohort were SuperAgers. Furthermore, because the criteria for SuperAging are fixed, maintaining SuperAger status can be tenuous following disease onset. Finally, this singular measure, developed by researchers, narrowly defines health in older age and maps irregularly onto the multifaceted lived experiences of dynamic aging.</p><p>Successful aging, described by Rowe and Kahn in 1987,<span><sup>6</sup></span> offered a positive multidimensional conceptual framework of aging, counter to the prevailing deficit-focused narrative of the time. Older adults are deemed Successful Agers if they meet three criteria: (a) avoid disease and disability; (b) maintain cognitive and physical function; and (c) engage with life through interpersonal relations and productive activity. Successful aging assumes that disease and disability are not inevitable and can be avoided, and cognitive and physical function maintained, through aggressive modification of risk. Studies examining factors associated with successful aging identified education, strenuous activity, peak pulmonary flow, self-efficacy, cultivating meaning, social engagement, optimal stress responses, and resilience as important to the maintenance of cognitive and physical function.<span><sup>7</sup></span> While embraced as a guiding gerontological theory since its inception, critics highlight potential stigma for those who experience disease, disability, and loss of cognitive and physical function. Moreover, nearly 40 years after its inception, Rowe and Kahn identified the need to conceptualize, examine, and address the impact of inequitable distribution of resources, systems that reinforce marginalization, and structural obstacles on an individual's potential for successful aging.<span><sup>7</sup></span> A broader approach is needed.</p><p>In essence, SuperAging and Successful Aging are aspirational—seeking to characterize a roadmap to unencumbered old age. However, as American poet laureate Donald Hall states, “old age is a ceremony of losses.”<span><sup>8</sup></span> Indeed, in the United States, 85% of people over 65 have at least one chronic condition, one-third have MCI or dementia, and one-third experience physical disability.<span><sup>9, 10</sup></span> Further, racial inequities persist across physical, cognitive, and functional impairments. We propose that it is time for an alternate framework of aging, Surviving Aging.</p><p>Surviving Aging differs from other models as it is grounded in the reality of aging for today's older Americans. It is an assets-based approach for <i>all</i> people as they age rather than for a few select aspirational agers. Assets are aspects of an individual's ecosystem that support achieving their goals and mitigate threats to their well-being throughout their lifetime. Assets can be conceptualized across the socioecological model at the individual, family, built and service, sociocultural, and political levels (Figure 1). In this paradigm, assets are unique to individuals and contexts, and outcomes are rooted in personal goals and values rather than being externally defined. Assets are dynamic—accumulating, changing, and diminishing over a person's life course based on their experiences and circumstances. Assets can be fostered in times of health, drawn upon, and even expanded in times of illness. Further, an assets-based model of aging can inform initiatives to address persistent health inequities by leveraging the strengths of communities rather than faultfinding.<span><sup>11</sup></span></p><p>An assets-based paradigm aims to accentuate positive capabilities, identify challenges, and activate solutions. Some studies show promise. CAPABLE, Positive Approach® to Care, and Daily Engagement of Meaningful Activities leverage assets to support the attainment of individualized goals (e.g., daily activities, interactions) for people with disability and/or cognitive impairment, impacting outcomes such as confidence, satisfaction, physical function, and depression.<span><sup>12-14</sup></span> To be sure, Surviving Aging demands an expanded menu of outcomes and factors relevant to all adults as they age, which can underpin research, clinical practice, and policy.</p><p>The Surviving Aging Framework needs further development. First, we need to clarify the theoretical basis and assumptions underlying Surviving Aging. Multiple disciplines (e.g., nursing, social work, psychology, occupational therapy) have lauded assets, but few describe the theoretical foundations of their approach. Salutogenesis offers a strong theoretical foundation for health creation rather than disease prevention.<span><sup>15, 16</sup></span> Second, we need methods of equitably identifying core health assets that are essential to older adults. Community asset mapping is an established participatory action method, grounded in health equity that is under-utilized in health research.<span><sup>17</sup></span> Third, we need to define cocreated assets-based outcomes with relevant partners, much like the efforts of LINC-AD. Finally, we need to evaluate the effectiveness of individual, family, community, system, and political approaches that support aging and address inequities.</p><p>Surviving Aging is a conceptual framework that is grounded in the lived experience of Americans facing the challenges of aging, cocreated with their input, and has the potential to support research, practice, and policy. Researchers will use the framework to conduct highly relevant and actionable research that generate fundamental insights into our understanding of what it means to age “well” in today's world. Clinicians can use the Surviving Aging Framework to identify each older American's goals (e.g., at an annual wellness visit), and assets (e.g., through asset mapping), and tailor their clinical efforts to align with both. Health systems, community-based organizations, and payers can cocreate care delivery and reimbursement models anchored to the outcomes that matter to aging Americans and that leverage the full range of assets available to individuals, communities, and organizations. After all, with activated aging assets, who needs a fountain of youth?</p><p><b>BEM</b>: Conceptualization, manuscript writing, reviewing, editing. <b>HM</b>: Conceptualization, manuscript writing, reviewing, editing. <b>DD</b>: Conceptualization, manuscript writing, reviewing, editing, supervision.</p><p>DD received support from the Cambia Health Foundation and National Palliative Care Research Center. BEM received support from NIA (NIA P30 AG066512).</p><p>None.</p><p>None.</p>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 10","pages":"2965-2968"},"PeriodicalIF":4.3000,"publicationDate":"2024-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11461098/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19126","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Rather than seeking time-bending bodies of water, today's scientists pursue the fountain of youth in older adults who demonstrate younger-than-expected attributes. SuperAgers, for example, exhibit signs of cognitive youth despite advanced age. Researchers seek to extract the fountain of youth from SuperAgers' modifiable risks. A 2020 Lancet Commission report found that addressing 12 modifiable risk factors could potentially prevent 40% of cases of dementia.2 While promising, this approach centers around combating aging rather than building upon its inherent assets and opportunities. In this editorial, we discuss the strengths and weaknesses of contemporary conceptual models of aging, highlight an article published in this issue that characterizes factors associated with SuperAgers in a sample of African Americans, and propose a new model of aging (Table 1). We aim to conceptualize an assets-based approach that incorporates both the strengths and challenges faced by all older adults seeking to survive aging.
SuperAging describes older adults who maintain cognitive function equal to normative middle-aged cohorts and is the guiding framework of the Trammel study. While some heterogeneity exists, SuperAging most frequently characterizes a person who is 80+ years old and performs extremely well on a measure of episodic memory (the Rey Auditory Verbal Learning Task), a single aspect of cognition. SuperAgers resist age-related changes (i.e., display cognitive resilience) and demonstrate neuroanatomical features of adults who are decades younger. The concept of SuperAgers is limited by exclusivity (median—12% of older adults), singular dimension (only episodic memory), and stigmatization for those who fail to meet the criteria.3, 4
Despite rising national awareness of racialized disparities in dementia, cognitive resilience in historically underrepresented racial and ethnic groups remains understudied. Using a nationally representative dataset, Trammel et al. explore differences among 1285 African American participants over 80 years old across three cohorts in the National Alzheimer's Coordinating Center dataset—SuperAgers, cognitively intact, and cognitively impaired. After accounting for gender and educational differences, classification as a SuperAger was associated with reduced prevalence of sleep disorders, decreased depression, and moderate alcohol usage. While SuperAgers exhibited vascular comorbidities comparable to non-SuperAgers, they were more likely to report taking medications, including antihypertensives and nonsteroidal anti-inflammatory drugs. Taken together, the results suggest that 80+-year-old African Americans who actively address chronic health conditions are most likely to demonstrate SuperAging status.
Research on SuperAgers has been a focus since 2012.5 It is quite remarkable that a study investigating SuperAgers in African American cohorts has not been conducted earlier. Applying aging frameworks to groups historically underrepresented in research (e.g., African American SuperAgers) can help to illuminate how well these frameworks integrate the experiences of all older adults. The strength of the SuperAging framework is its specificity. Inclusion is a single concrete measure with a defined threshold. However, while SuperAging reveals the remarkable capacity of older adults, very few will attain this status. A mere 4.7% of the sample in Trammel's cohort were SuperAgers. Furthermore, because the criteria for SuperAging are fixed, maintaining SuperAger status can be tenuous following disease onset. Finally, this singular measure, developed by researchers, narrowly defines health in older age and maps irregularly onto the multifaceted lived experiences of dynamic aging.
Successful aging, described by Rowe and Kahn in 1987,6 offered a positive multidimensional conceptual framework of aging, counter to the prevailing deficit-focused narrative of the time. Older adults are deemed Successful Agers if they meet three criteria: (a) avoid disease and disability; (b) maintain cognitive and physical function; and (c) engage with life through interpersonal relations and productive activity. Successful aging assumes that disease and disability are not inevitable and can be avoided, and cognitive and physical function maintained, through aggressive modification of risk. Studies examining factors associated with successful aging identified education, strenuous activity, peak pulmonary flow, self-efficacy, cultivating meaning, social engagement, optimal stress responses, and resilience as important to the maintenance of cognitive and physical function.7 While embraced as a guiding gerontological theory since its inception, critics highlight potential stigma for those who experience disease, disability, and loss of cognitive and physical function. Moreover, nearly 40 years after its inception, Rowe and Kahn identified the need to conceptualize, examine, and address the impact of inequitable distribution of resources, systems that reinforce marginalization, and structural obstacles on an individual's potential for successful aging.7 A broader approach is needed.
In essence, SuperAging and Successful Aging are aspirational—seeking to characterize a roadmap to unencumbered old age. However, as American poet laureate Donald Hall states, “old age is a ceremony of losses.”8 Indeed, in the United States, 85% of people over 65 have at least one chronic condition, one-third have MCI or dementia, and one-third experience physical disability.9, 10 Further, racial inequities persist across physical, cognitive, and functional impairments. We propose that it is time for an alternate framework of aging, Surviving Aging.
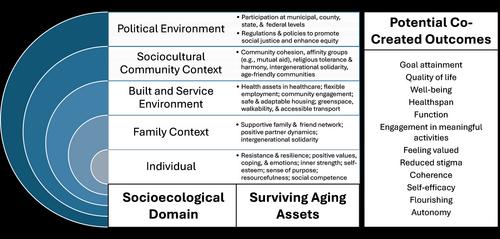
Surviving Aging differs from other models as it is grounded in the reality of aging for today's older Americans. It is an assets-based approach for all people as they age rather than for a few select aspirational agers. Assets are aspects of an individual's ecosystem that support achieving their goals and mitigate threats to their well-being throughout their lifetime. Assets can be conceptualized across the socioecological model at the individual, family, built and service, sociocultural, and political levels (Figure 1). In this paradigm, assets are unique to individuals and contexts, and outcomes are rooted in personal goals and values rather than being externally defined. Assets are dynamic—accumulating, changing, and diminishing over a person's life course based on their experiences and circumstances. Assets can be fostered in times of health, drawn upon, and even expanded in times of illness. Further, an assets-based model of aging can inform initiatives to address persistent health inequities by leveraging the strengths of communities rather than faultfinding.11
An assets-based paradigm aims to accentuate positive capabilities, identify challenges, and activate solutions. Some studies show promise. CAPABLE, Positive Approach® to Care, and Daily Engagement of Meaningful Activities leverage assets to support the attainment of individualized goals (e.g., daily activities, interactions) for people with disability and/or cognitive impairment, impacting outcomes such as confidence, satisfaction, physical function, and depression.12-14 To be sure, Surviving Aging demands an expanded menu of outcomes and factors relevant to all adults as they age, which can underpin research, clinical practice, and policy.
The Surviving Aging Framework needs further development. First, we need to clarify the theoretical basis and assumptions underlying Surviving Aging. Multiple disciplines (e.g., nursing, social work, psychology, occupational therapy) have lauded assets, but few describe the theoretical foundations of their approach. Salutogenesis offers a strong theoretical foundation for health creation rather than disease prevention.15, 16 Second, we need methods of equitably identifying core health assets that are essential to older adults. Community asset mapping is an established participatory action method, grounded in health equity that is under-utilized in health research.17 Third, we need to define cocreated assets-based outcomes with relevant partners, much like the efforts of LINC-AD. Finally, we need to evaluate the effectiveness of individual, family, community, system, and political approaches that support aging and address inequities.
Surviving Aging is a conceptual framework that is grounded in the lived experience of Americans facing the challenges of aging, cocreated with their input, and has the potential to support research, practice, and policy. Researchers will use the framework to conduct highly relevant and actionable research that generate fundamental insights into our understanding of what it means to age “well” in today's world. Clinicians can use the Surviving Aging Framework to identify each older American's goals (e.g., at an annual wellness visit), and assets (e.g., through asset mapping), and tailor their clinical efforts to align with both. Health systems, community-based organizations, and payers can cocreate care delivery and reimbursement models anchored to the outcomes that matter to aging Americans and that leverage the full range of assets available to individuals, communities, and organizations. After all, with activated aging assets, who needs a fountain of youth?
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


