{"title":"Exporting nuclear export inhibitors from hematologic to solid tumour malignancies","authors":"Alexandra Chirino, Alyssa Maye, Justin Taylor","doi":"10.1002/ctd2.356","DOIUrl":null,"url":null,"abstract":"<p>Exportin 1 (XPO1), formerly known as chromosomal region maintenance 1, belongs to the karyopherin family of proteins that are responsible for the import and export of macromolecules through the nuclear pore complex. XPO1 is the sole exporter of hundreds of cargoes including several RNA species and key proteins such as tumor suppressors and cell cycle proteins. Despite its essential and housekeeping function in normal cells, in their review, Lai et al note that upregulation of XPO1 is associated with a wide variety of cancers, including but not limited to colorectal cancer, osteosarcoma, lung cancer, gastric cancer, ovarian cancer, glioma, pancreatic cancer and oesophagal cancer.<span><sup>1</sup></span> In non-cancer cells, XPO1 shuttles RNA and proteins from the nucleus to the cytoplasm while also regulating mitosis during interphase. After performing its export function, XPO1 returns to the nucleus to repeat the process, making it a vital part of sustaining normal cellular physiological functions (Figure 1). However, increased expression of XPO1 leads to increased export and imbalance of nucleo-cytoplasmic transport.</p><p>Though the exact mechanisms regulating the overexpression of XPO1 in solid cancers are not yet completely understood, chromosome 2p amplification accounts for this in a subset of hematologic neoplasms. Another means of dysregulation of XPO1 that is found in hematologic malignancies is the missense mutation <i>XPO1</i> E517K, which has been linked to facilitating the growth of malignant B cells in chronic lymphocytic leukaemia and Hodgkin lymphoma.<span><sup>2</sup></span> Clinical trials of XPO1 inhibitors in hematologic malignancies have shown response rates ranging from 26% to 45% in those with advanced multiple myeloma, and a 28% response rate in those with relapsed or refractory diffuse large B cell lymphoma.<span><sup>3-5</sup></span> Due to this success, selinexor, the first-in-class XPO1 inhibitor has been Food and Drug Administration-approved for these two indications.</p><p>This leads to the big question—can targeting XPO1 be successful in solid tumours? According to Lai et al, while promising, it comes with considerable challenges. The first XPO1 inhibitors were natural products that irreversibly bound XPO1 and caused severe toxic side effects, leading to the discontinuation of their development as anticancer therapies. In response, small molecule XPO1 inhibitors were designed to be slowly reversible and are more tolerable in patients. Preclinical data suggests that selinexor is active in tumours with previous drug resistance in vitro and in vivo and induces apoptosis in many cancerous cell lines including but not limited to prostate, bladder, and renal cell carcinoma. While reducing the tumour is the main goal for these preclinical studies, there are questions of dose dependency for cancers like sarcomas, which may not be feasible for humans in clinical trials.<span><sup>6</sup></span> However, that is not to diminish the importance of these studies, as they can give us further insights. One study suggested KRAS mutant lung cancer was dependent on XPO1 as the KRAS mutant line could not handle the buildup of nuclear IκBα once nuclear export was inhibited, pinpointing a critical mechanism of action.<span><sup>7</sup></span> Other studies show the potential of combination therapies, such as a glioblastoma study that found high synergistic effects with bortezomib, dactinomycin, or vinorelbine. With such evidence, selinexor has begun various clinical trials in solid tumours.</p><p>Lai et al. describe the results of selinexor clinical trials across several types of solid cancers. Currently, there are 58 different studies involving selinexor that are recruiting or active, and 35 completed trials. Of note, an open phase II glioblastoma trial has shown success with selinexor, with an overall group rate of 28% tumour reduction and only 34% reporting adverse effects (AEs). One of the groups given the lowest dose per week had an overall response rate of 10% while also having the highest 6-month progression-free survival at 17.7%.<span><sup>8</sup></span> Another study in gynaecological cancers showed 38% tumour reduction, and 7% reaching partial response for about 7.4 months.<span><sup>9</sup></span> A double-blind phase III trial of selinexor for endometrial cancer is underway (NCT03555422) and if successful, may lead to the first approval of selinexor for solid tumors. On the other hand, there are 16 or so trials which were terminated due to both adverse side effects and selinexor failing to meet trial expectations, further emphasizing the need for more studies, and possibly more research into other XPO1 inhibitors, such as second-generation eltanexor. So far, eltanexor has shown less blood-brain barrier penetration and weight loss in animal models when compared to selinexor and is currently going under a phase I trial to see its effects in patients (NCT02649790). Felezonexor, another XPO1 inhibitor, also completed a phase I study to determine effects as well as dosage in patients with solid tumours specifically (NCT02667873), with previous results showing the best response of stable disease.<span><sup>10</sup></span></p><p>Given the above, selinexor may be worth continuing to pursue in solid tumours; however, the ratio of successful to terminated trials suggests that future clinical trials need to be more targeted to populations most likely to respond to XPO1 inhibition. Another obstacle to grapple with is the AEs, with more studies needed to find the minimum dose needed for efficacy. A minimal low-effective dose of selinexor may then be added to other treatments with high synergetic effects. Further studies may allow for a better understanding of which patients can benefit most from this treatment.</p><p>Alexandra Chirino and Justin Taylor conceptualized the manuscript. Alexandra Chirino and Alyssa Maye wrote the first draft of the manuscript. Justin Taylor revised and wrote the final draft of the manuscript. All authors approve of the final draft.</p><p>The authors declare no conflict of interest.</p><p>Not applicable.</p>","PeriodicalId":72605,"journal":{"name":"Clinical and translational discovery","volume":"4 4","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ctd2.356","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and translational discovery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ctd2.356","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
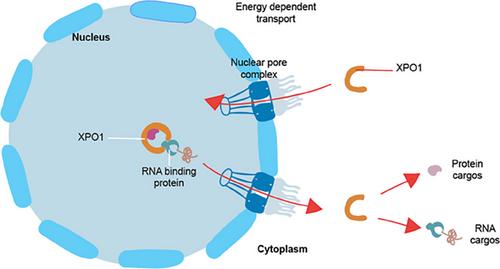
Exportin 1 (XPO1), formerly known as chromosomal region maintenance 1, belongs to the karyopherin family of proteins that are responsible for the import and export of macromolecules through the nuclear pore complex. XPO1 is the sole exporter of hundreds of cargoes including several RNA species and key proteins such as tumor suppressors and cell cycle proteins. Despite its essential and housekeeping function in normal cells, in their review, Lai et al note that upregulation of XPO1 is associated with a wide variety of cancers, including but not limited to colorectal cancer, osteosarcoma, lung cancer, gastric cancer, ovarian cancer, glioma, pancreatic cancer and oesophagal cancer.1 In non-cancer cells, XPO1 shuttles RNA and proteins from the nucleus to the cytoplasm while also regulating mitosis during interphase. After performing its export function, XPO1 returns to the nucleus to repeat the process, making it a vital part of sustaining normal cellular physiological functions (Figure 1). However, increased expression of XPO1 leads to increased export and imbalance of nucleo-cytoplasmic transport.
Though the exact mechanisms regulating the overexpression of XPO1 in solid cancers are not yet completely understood, chromosome 2p amplification accounts for this in a subset of hematologic neoplasms. Another means of dysregulation of XPO1 that is found in hematologic malignancies is the missense mutation XPO1 E517K, which has been linked to facilitating the growth of malignant B cells in chronic lymphocytic leukaemia and Hodgkin lymphoma.2 Clinical trials of XPO1 inhibitors in hematologic malignancies have shown response rates ranging from 26% to 45% in those with advanced multiple myeloma, and a 28% response rate in those with relapsed or refractory diffuse large B cell lymphoma.3-5 Due to this success, selinexor, the first-in-class XPO1 inhibitor has been Food and Drug Administration-approved for these two indications.
This leads to the big question—can targeting XPO1 be successful in solid tumours? According to Lai et al, while promising, it comes with considerable challenges. The first XPO1 inhibitors were natural products that irreversibly bound XPO1 and caused severe toxic side effects, leading to the discontinuation of their development as anticancer therapies. In response, small molecule XPO1 inhibitors were designed to be slowly reversible and are more tolerable in patients. Preclinical data suggests that selinexor is active in tumours with previous drug resistance in vitro and in vivo and induces apoptosis in many cancerous cell lines including but not limited to prostate, bladder, and renal cell carcinoma. While reducing the tumour is the main goal for these preclinical studies, there are questions of dose dependency for cancers like sarcomas, which may not be feasible for humans in clinical trials.6 However, that is not to diminish the importance of these studies, as they can give us further insights. One study suggested KRAS mutant lung cancer was dependent on XPO1 as the KRAS mutant line could not handle the buildup of nuclear IκBα once nuclear export was inhibited, pinpointing a critical mechanism of action.7 Other studies show the potential of combination therapies, such as a glioblastoma study that found high synergistic effects with bortezomib, dactinomycin, or vinorelbine. With such evidence, selinexor has begun various clinical trials in solid tumours.
Lai et al. describe the results of selinexor clinical trials across several types of solid cancers. Currently, there are 58 different studies involving selinexor that are recruiting or active, and 35 completed trials. Of note, an open phase II glioblastoma trial has shown success with selinexor, with an overall group rate of 28% tumour reduction and only 34% reporting adverse effects (AEs). One of the groups given the lowest dose per week had an overall response rate of 10% while also having the highest 6-month progression-free survival at 17.7%.8 Another study in gynaecological cancers showed 38% tumour reduction, and 7% reaching partial response for about 7.4 months.9 A double-blind phase III trial of selinexor for endometrial cancer is underway (NCT03555422) and if successful, may lead to the first approval of selinexor for solid tumors. On the other hand, there are 16 or so trials which were terminated due to both adverse side effects and selinexor failing to meet trial expectations, further emphasizing the need for more studies, and possibly more research into other XPO1 inhibitors, such as second-generation eltanexor. So far, eltanexor has shown less blood-brain barrier penetration and weight loss in animal models when compared to selinexor and is currently going under a phase I trial to see its effects in patients (NCT02649790). Felezonexor, another XPO1 inhibitor, also completed a phase I study to determine effects as well as dosage in patients with solid tumours specifically (NCT02667873), with previous results showing the best response of stable disease.10
Given the above, selinexor may be worth continuing to pursue in solid tumours; however, the ratio of successful to terminated trials suggests that future clinical trials need to be more targeted to populations most likely to respond to XPO1 inhibition. Another obstacle to grapple with is the AEs, with more studies needed to find the minimum dose needed for efficacy. A minimal low-effective dose of selinexor may then be added to other treatments with high synergetic effects. Further studies may allow for a better understanding of which patients can benefit most from this treatment.
Alexandra Chirino and Justin Taylor conceptualized the manuscript. Alexandra Chirino and Alyssa Maye wrote the first draft of the manuscript. Justin Taylor revised and wrote the final draft of the manuscript. All authors approve of the final draft.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


