Robert Rainer, Blair Creedle Reynolds, Cyrus Adeli, Christopher E San Miguel
{"title":"Subarachnoid Hemorrhage Causing a Seizure: An Assessment Simulation for Medical Students.","authors":"Robert Rainer, Blair Creedle Reynolds, Cyrus Adeli, Christopher E San Miguel","doi":"10.21980/J8XH1H","DOIUrl":null,"url":null,"abstract":"<p><strong>Audience: </strong>This simulation is intended for 4<sup>th</sup> year medical students.</p><p><strong>Introduction: </strong>Headache is the fifth most common chief complaint in the emergency room, and the vast majority are ultimately diagnosed as benign primary headaches.1,2 However, subarachnoid hemorrhage (SAH) is one of several critical diagnoses which can present as a headache. With a case fatality rate of up to 66.7% in some instances, SAH is considered a \"can't miss\" diagnosis.3Subarachnoid hemorrhage is classically associated with a thunderclap headache, one definition of which is a headache that reaches maximal intensity within one minute or less and reaches a seven out of ten in severity.1 Unfortunately, a thunderclap headache is not as sensitive nor specific for SAH as is often taught. In one study, only 50% of patients with an aneurysmal subarachnoid hemorrhage presented with a thunderclap headache and an additional 19% of SAH headache came on more gradually over the course of five minutes.4 A second study found that only 66% of SAH patients reported a thunderclap headache.2 Thunderclap headaches can also be associated with other intercranial pathology including intracerebral hemorrhage, cerebral venous thrombosis, cervical artery dissection, posterior reversible encephalopathy syndrome, meningitis, and temporal arteritis among others.1,2 In a large observational study, SAH accounted for 32% of the serious pathology cases identified in patients with a thunderclap headache. Even among the thunderclap headache cohort, however, 88% of patients ultimately had a benign diagnosis (compared to 93% of patients who did not report a thunderclap headache).2Additional signs and symptoms of SAH include seizures in 6-9% of patients, vomiting, neck pain and stiffness, visual disturbances, loss of consciousness, and focal cranial nerve or supratentorial deficits.1,5 A non-contrasted computer tomography (CT) of the head within six hours of headache onset can have a sensitivity of 98.7 to 100%; however, the sensitivity decreased to 86% at the 24-48 hour mark.1,6 A meta-analysis found a pooled six hour sensitivity of 1.0 and asserts that a head CT interpreted as negative by an attending radiologist effectively rules out SAH in neurologically intact patients with a defined onset of a thunderclap headache.6 Some guidelines in the United States still recommend shared decision making with the patient to choose between a Lumbar Puncture (LP), Computer Tomography Angiogram (CTA), or no further testing to rule out SAH in the case of a negative head CT.2 The more time that has elapsed between onset and CT imaging, the stronger the recommendation to pursue further testing. A negative head CT followed by a negative LP approaches 100% sensitivity for ruling out SAH, and a negative head CT with a negative CTA has a 99.4% probability of ruling out SAH.1,3 Thus it is an important learning point that if a headache has been ongoing for more than six hours and there is a high pre-test probability for an SAH, a negative head CT is not sufficient to rule out the diagnosis, and a secondary test should be ordered.Status epilepticus is defined as five minutes of continuous seizure activity or repeated seizures without return to baseline between seizures.7 The immediate priorities for a seizing patient include providing supplemental oxygen, considering intubation if patient is unable to protect airway, obtaining IV access if not previously established, and checking glucose.7 The main priority for a patient in status epilepticus is to stop the seizure with seizure abortive medications, typically benzodiazepines, and treat life-threatening causes of status epilepticus.7 This simulation will enable learners to diagnose SAH that is not the classical \"worst headache of my life\" and manage an actively seizing patient.</p><p><strong>Educational objectives: </strong>At the conclusion of the simulation leaners will be able to:Efficiently take a history from the patient and perform a physical exam (including a complete neurological exam)Identify red flag symptoms in a patient complaining of a headacheOrder and interpret the results of a CT of the head and either a CT angiogram of the brain or a lumbar puncture to make the diagnosis of subarachnoid hemorrhageDemonstrate appropriate management of a seizureCheck a fingerstick glucoseProvide supplemental oxygenAdminister an IV or IM benzodiazepine to treat the seizureUtilize the I-PASS framework to communicate with the inpatient team during the transition of care.</p><p><strong>Educational methods: </strong>This summative simulation was designed to assess competence in two of the core Entrustable Professional Activities (EPAs), as defined by the Association of American Medical Colleges (AAMC). These include EPA 8 (Give or Receive a Patient Handover to Transition Care Responsibility) and EPA 10 (Recognize a Patient Requiring Urgent or Emergent Care and Initiate Evaluation and Management). It was performed with 4th year medical students at the conclusion of their required month-long emergency medicine (EM) clerkship. This scenario joined eight other scenarios in our pool of potential cases. These sessions are conducted using a high-fidelity manikin as the patient and a confederate/actor in the nursing role. The students complete the assessment in groups of three or four with each student acting as the team lead for one scenario. After each scenario concludes, there is a post-simulation debriefing session on the presentation, differential diagnosis, physical exam findings, and management of the target pathology. A Gather-Analyze-Summarize technique was used for the debriefing session.8.</p><p><strong>Research methods: </strong>Facilitators provided informal feedback to the scenario developers after the case was introduced into the assessment rotation. Learners completed a standard evaluation issued by the College of Medicine for the entire session rather than for individual scenarios. These evaluations were reviewed for the first year of implementation of this new case. Over the year, 209 students completed the summative simulation exercise, and 84 of those students completed this simulation as part of the overall exercise.</p><p><strong>Results: </strong>Overall, our facilitators felt the case fit well into our pool of simulation cases. They felt they were adequately able to assess the students' ability to respond to a seizing patient and thought the difficulty level was appropriate for fourth year medical students. Students are asked to assess the simulation session as a whole using a standard evaluation form from the College of Medicine. The simulation assessment exercise as a whole was highly rated by the students, with 93% of students rating the overall quality of the session as Very Good or Excellent. Of the students who completed the SAH scenario, 96% rated the overall quality of the session as Very Good or Excellent. None of the comments specifically mention the SAH case.</p><p><strong>Discussion: </strong>Our department has run formative simulations during the 4th year EM clerkship for over ten years. Our primary objective is to assess 4th year students' competence in EPA 10 (Recognize a Patient Requiring Urgent or Emergent Care and Initiate Evaluation and Management). This simulation case was written to replace another SAH case which was a more straightforward and typical presentation of a subarachnoid hemorrhage as \"the worst headache of my life.\" The previous case also did not require seizure management. The inclusion of the seizure management better allowed faculty to assess the students' response to a patient's acute decompensation, which is more in line with EPA 10, than simply making a critical diagnosis.Our facilitators did notice that many groups initially work the patient up for meningitis but ultimately make the correct diagnosis with the lumbar puncture (LP) results. Because the students have correctly identified that the patient requires more extensive work up, and meningitis is certainly on the differential diagnoses, students are not penalized for following this line of clinical reasoning.This simulation proved to be highly engaging for 4th year medical students, and students seemed to perform at a similar level as previous summative simulations. Overall, we felt this simulation successfully achieved the objectives of the simulation session as whole, and it was integrated into our 4th year EM clerkship simulation curriculum.</p><p><strong>Topics: </strong>Medical simulation, Emergency Medicine, Subarachnoid Hemorrhage, Intracranial Hemorrhage, Seizure, Status Epilepticus.</p>","PeriodicalId":73721,"journal":{"name":"Journal of education & teaching in emergency medicine","volume":"9 3","pages":"S30-S64"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11312874/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of education & teaching in emergency medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21980/J8XH1H","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Audience: This simulation is intended for 4th year medical students.
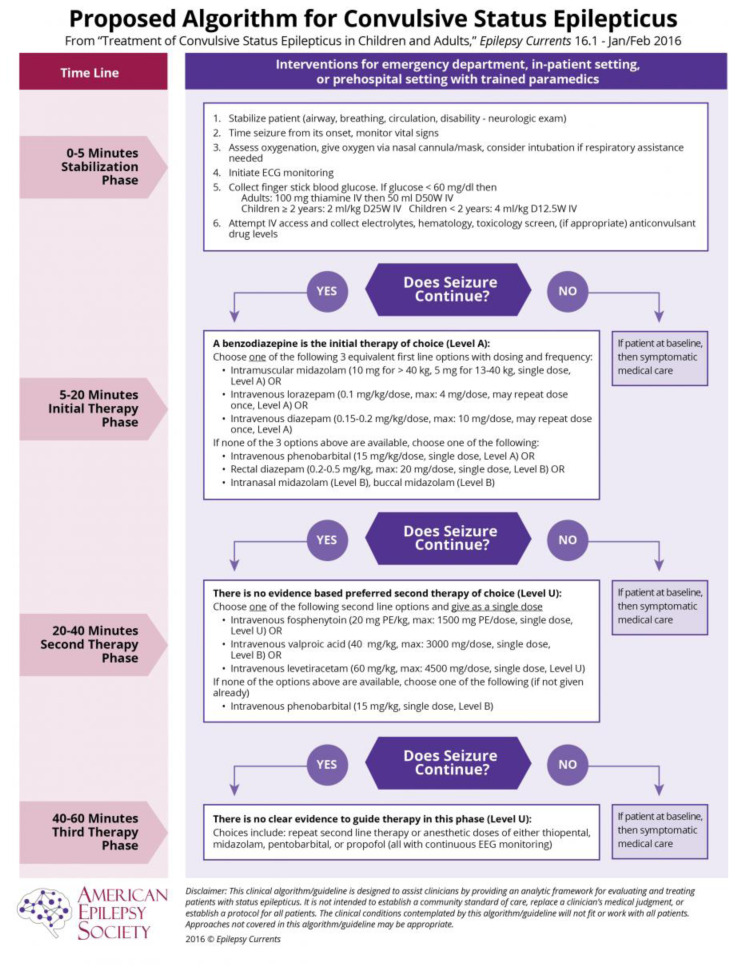
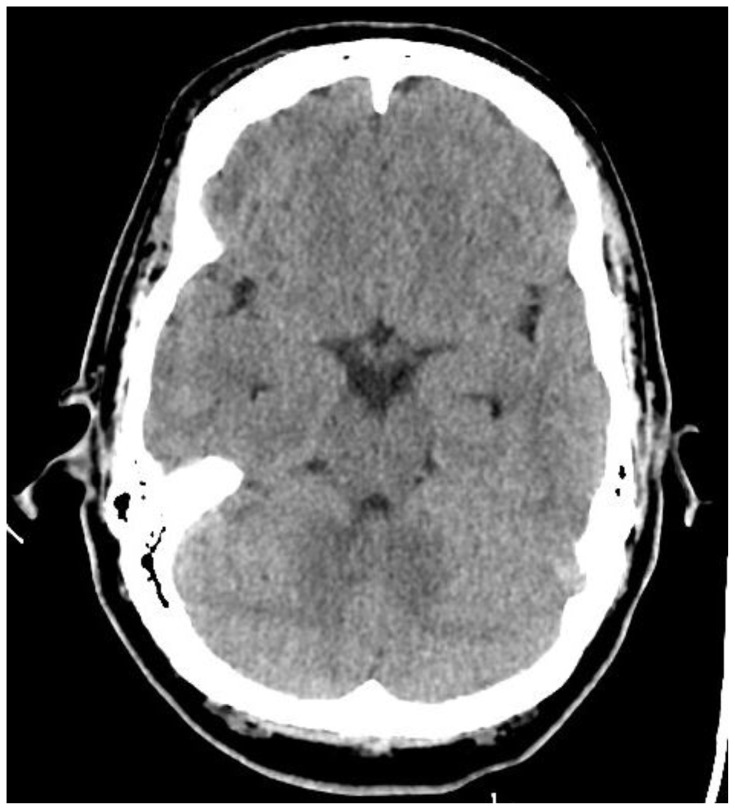
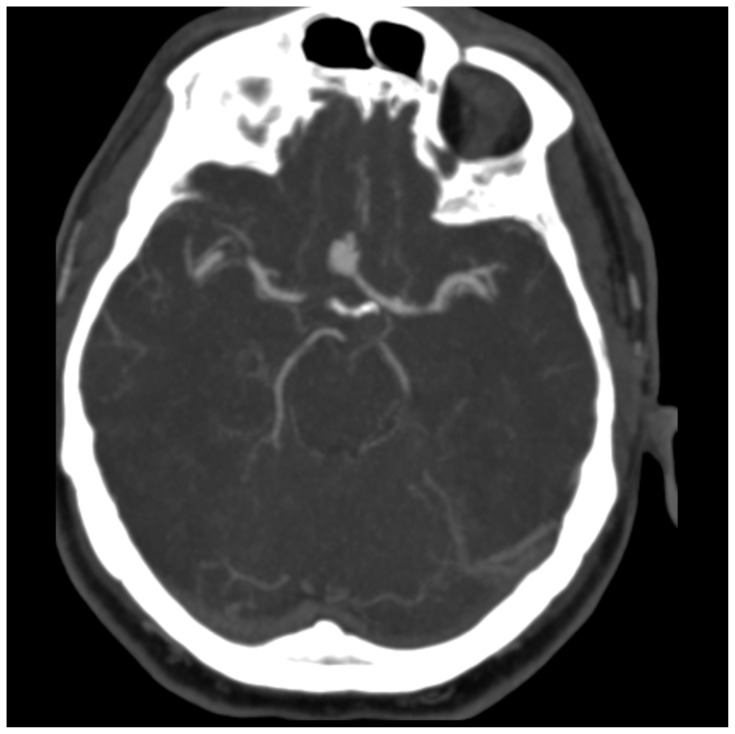
Introduction: Headache is the fifth most common chief complaint in the emergency room, and the vast majority are ultimately diagnosed as benign primary headaches.1,2 However, subarachnoid hemorrhage (SAH) is one of several critical diagnoses which can present as a headache. With a case fatality rate of up to 66.7% in some instances, SAH is considered a "can't miss" diagnosis.3Subarachnoid hemorrhage is classically associated with a thunderclap headache, one definition of which is a headache that reaches maximal intensity within one minute or less and reaches a seven out of ten in severity.1 Unfortunately, a thunderclap headache is not as sensitive nor specific for SAH as is often taught. In one study, only 50% of patients with an aneurysmal subarachnoid hemorrhage presented with a thunderclap headache and an additional 19% of SAH headache came on more gradually over the course of five minutes.4 A second study found that only 66% of SAH patients reported a thunderclap headache.2 Thunderclap headaches can also be associated with other intercranial pathology including intracerebral hemorrhage, cerebral venous thrombosis, cervical artery dissection, posterior reversible encephalopathy syndrome, meningitis, and temporal arteritis among others.1,2 In a large observational study, SAH accounted for 32% of the serious pathology cases identified in patients with a thunderclap headache. Even among the thunderclap headache cohort, however, 88% of patients ultimately had a benign diagnosis (compared to 93% of patients who did not report a thunderclap headache).2Additional signs and symptoms of SAH include seizures in 6-9% of patients, vomiting, neck pain and stiffness, visual disturbances, loss of consciousness, and focal cranial nerve or supratentorial deficits.1,5 A non-contrasted computer tomography (CT) of the head within six hours of headache onset can have a sensitivity of 98.7 to 100%; however, the sensitivity decreased to 86% at the 24-48 hour mark.1,6 A meta-analysis found a pooled six hour sensitivity of 1.0 and asserts that a head CT interpreted as negative by an attending radiologist effectively rules out SAH in neurologically intact patients with a defined onset of a thunderclap headache.6 Some guidelines in the United States still recommend shared decision making with the patient to choose between a Lumbar Puncture (LP), Computer Tomography Angiogram (CTA), or no further testing to rule out SAH in the case of a negative head CT.2 The more time that has elapsed between onset and CT imaging, the stronger the recommendation to pursue further testing. A negative head CT followed by a negative LP approaches 100% sensitivity for ruling out SAH, and a negative head CT with a negative CTA has a 99.4% probability of ruling out SAH.1,3 Thus it is an important learning point that if a headache has been ongoing for more than six hours and there is a high pre-test probability for an SAH, a negative head CT is not sufficient to rule out the diagnosis, and a secondary test should be ordered.Status epilepticus is defined as five minutes of continuous seizure activity or repeated seizures without return to baseline between seizures.7 The immediate priorities for a seizing patient include providing supplemental oxygen, considering intubation if patient is unable to protect airway, obtaining IV access if not previously established, and checking glucose.7 The main priority for a patient in status epilepticus is to stop the seizure with seizure abortive medications, typically benzodiazepines, and treat life-threatening causes of status epilepticus.7 This simulation will enable learners to diagnose SAH that is not the classical "worst headache of my life" and manage an actively seizing patient.
Educational objectives: At the conclusion of the simulation leaners will be able to:Efficiently take a history from the patient and perform a physical exam (including a complete neurological exam)Identify red flag symptoms in a patient complaining of a headacheOrder and interpret the results of a CT of the head and either a CT angiogram of the brain or a lumbar puncture to make the diagnosis of subarachnoid hemorrhageDemonstrate appropriate management of a seizureCheck a fingerstick glucoseProvide supplemental oxygenAdminister an IV or IM benzodiazepine to treat the seizureUtilize the I-PASS framework to communicate with the inpatient team during the transition of care.
Educational methods: This summative simulation was designed to assess competence in two of the core Entrustable Professional Activities (EPAs), as defined by the Association of American Medical Colleges (AAMC). These include EPA 8 (Give or Receive a Patient Handover to Transition Care Responsibility) and EPA 10 (Recognize a Patient Requiring Urgent or Emergent Care and Initiate Evaluation and Management). It was performed with 4th year medical students at the conclusion of their required month-long emergency medicine (EM) clerkship. This scenario joined eight other scenarios in our pool of potential cases. These sessions are conducted using a high-fidelity manikin as the patient and a confederate/actor in the nursing role. The students complete the assessment in groups of three or four with each student acting as the team lead for one scenario. After each scenario concludes, there is a post-simulation debriefing session on the presentation, differential diagnosis, physical exam findings, and management of the target pathology. A Gather-Analyze-Summarize technique was used for the debriefing session.8.
Research methods: Facilitators provided informal feedback to the scenario developers after the case was introduced into the assessment rotation. Learners completed a standard evaluation issued by the College of Medicine for the entire session rather than for individual scenarios. These evaluations were reviewed for the first year of implementation of this new case. Over the year, 209 students completed the summative simulation exercise, and 84 of those students completed this simulation as part of the overall exercise.
Results: Overall, our facilitators felt the case fit well into our pool of simulation cases. They felt they were adequately able to assess the students' ability to respond to a seizing patient and thought the difficulty level was appropriate for fourth year medical students. Students are asked to assess the simulation session as a whole using a standard evaluation form from the College of Medicine. The simulation assessment exercise as a whole was highly rated by the students, with 93% of students rating the overall quality of the session as Very Good or Excellent. Of the students who completed the SAH scenario, 96% rated the overall quality of the session as Very Good or Excellent. None of the comments specifically mention the SAH case.
Discussion: Our department has run formative simulations during the 4th year EM clerkship for over ten years. Our primary objective is to assess 4th year students' competence in EPA 10 (Recognize a Patient Requiring Urgent or Emergent Care and Initiate Evaluation and Management). This simulation case was written to replace another SAH case which was a more straightforward and typical presentation of a subarachnoid hemorrhage as "the worst headache of my life." The previous case also did not require seizure management. The inclusion of the seizure management better allowed faculty to assess the students' response to a patient's acute decompensation, which is more in line with EPA 10, than simply making a critical diagnosis.Our facilitators did notice that many groups initially work the patient up for meningitis but ultimately make the correct diagnosis with the lumbar puncture (LP) results. Because the students have correctly identified that the patient requires more extensive work up, and meningitis is certainly on the differential diagnoses, students are not penalized for following this line of clinical reasoning.This simulation proved to be highly engaging for 4th year medical students, and students seemed to perform at a similar level as previous summative simulations. Overall, we felt this simulation successfully achieved the objectives of the simulation session as whole, and it was integrated into our 4th year EM clerkship simulation curriculum.
Topics: Medical simulation, Emergency Medicine, Subarachnoid Hemorrhage, Intracranial Hemorrhage, Seizure, Status Epilepticus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


