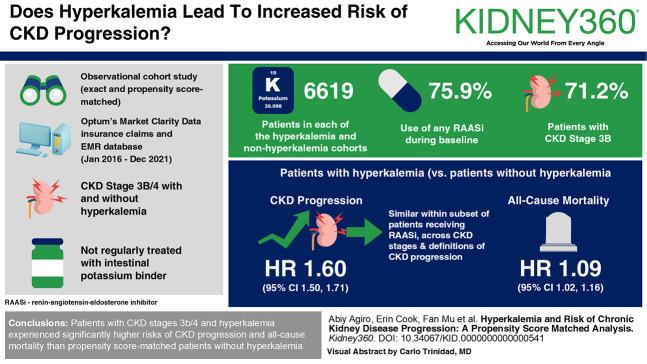
Hyperkalemia and Risk of CKD Progression: A Propensity Score-Matched Analysis.
IF 3
Q1 UROLOGY & NEPHROLOGY
引用次数: 0
高钾血症与慢性肾病恶化的风险:倾向得分匹配分析
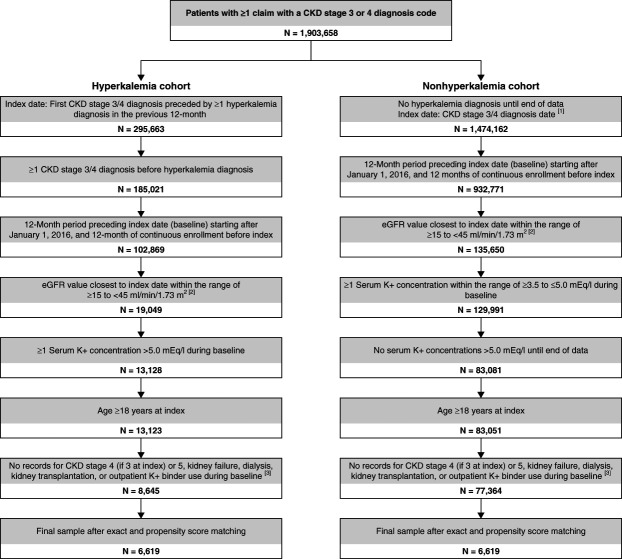
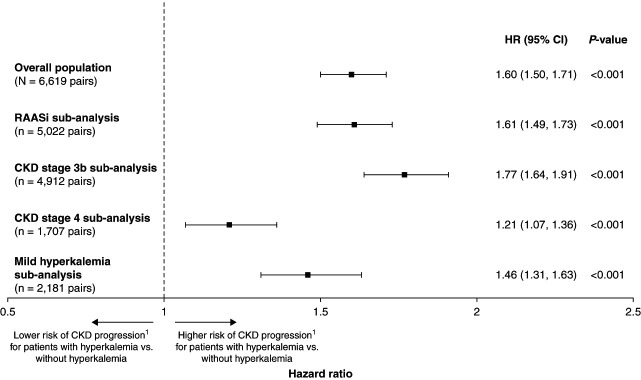
背景:众所周知,高钾血症是慢性肾脏病(CKD)的一种并发症;但是,高钾血症是否直接导致了 CKD 的进展和死亡风险,目前尚不清楚。明确高钾血症与 CKD 进展和死亡的相关程度可为临床实践提供依据并指导未来的研究。本研究的目的是量化 3b/4 期慢性肾脏病患者中与高钾血症相关的慢性肾脏病进展和死亡风险:这是一项真实世界、精确和倾向得分匹配的观察性队列研究,使用的数据(2016 年 1 月至 2021 年 12 月)来自 Optum 的去标识化 Market Clarity 数据,这是一个大型的美国综合保险索赔/电子病历数据库。研究对象包括伴有或不伴有高钾血症的 3b/4 期慢性肾功能衰竭成人患者,这些患者未定期接受肠钾 (K+) 结合剂治疗。测量结果为慢性肾功能衰竭进展和全因死亡率。CKD进展的定义是诊断为CKD 4期(如果指数为3b期)、CKD 5期或肾衰竭,或接受透析或肾移植:配对后,高钾血症组和非高钾血症组各有 6619 名患者,平均(标准差)随访时间为 2.12(1.42)年。基线期间使用任何肾素-血管紧张素-醛固酮系统抑制剂(RAASi)的情况很普遍(75.9%),大多数患者处于慢性肾脏病 3b 期(71.2%)。与没有高钾血症的患者相比,高钾血症患者的 CKD 进展风险高 1.60 倍(95% 置信区间 [CI] 1.50,1.71),全因死亡风险高 1.09 倍(1.02,1.16)。在接受RAASi治疗的亚组患者中,以及在不同CKD分期和使用其他CKD进展定义时,与高钾血症相关的CKD进展相对风险相似:结论:与没有高钾血症的倾向评分匹配患者相比,CKD 3b/4 期和高钾血症患者的 CKD 进展风险和全因死亡率明显更高。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


