{"title":"WEO Newsletter: Tips and tricks: Assessment and endoscopic dilation of strictures in inflammatory bowel disease (IBD)","authors":"","doi":"10.1111/den.14902","DOIUrl":null,"url":null,"abstract":"<p>Gursimran S. Kochhar, MD, is a gastroenterologist, Division Chief of the Department of Gastroenterology and Hepatology, at Allegheny Health Network, Pittsburgh, Pennsylvania. He specializes in interventional inflammatory bowel disease (IBD) and advanced therapeutic procedures.</p><p>Dr. Kochhar completed his training in internal medicine at Cleveland Clinic Foundation, Cleveland, Ohio, where he subsequently received training in nutrition and finished a gastroenterology and hepatology fellowship focused on training in IBD. Dr. Kochhar then completed his advanced endoscopy fellowship at Mayo Clinic, Jacksonville, Florida.</p><p>Dr. Kochhar has been at the forefront of managing IBD and its complications with various advanced endoscopic procedures. His innovative research on the endoscopic management of IBD has been successfully published in leading gastroenterology journals, including Gastroenterology, Clinical Gastroenterology and Hepatology, and Gastrointestinal Endoscopy. He has more than 120 publications, including peer-reviewed articles and book chapters. He serves on the Editorial Board of the journal Inflammatory Bowel Diseases. His current research focuses on endoscopic management of IBD complications, artificial intelligence in health care, and newer endoscopic innovations.</p><p>Stricture formation is a common complication in Crohn's disease (CD) patients, resulting from the underlying disease process, surgical anastomosis, or strictureplasty. The true incidence of stricturing disease is hard to assess. However, some studies suggest the prevalence of strictures is up to 25% in patients with CD, and over 50% of patients with CD will need at least one surgery in their lifetime.</p><p>Endoscopic balloon dilation (EBD), first described by Dr. G.M. Heller in 1988 in a patient with CD,1 is a very important tool in our toolbox to manage strictures in such patients. EBD, if done well, can be very effective in mitigating or delaying surgeries in patients with CD (Fig. 1).</p><p>Endoscopic assessment of strictures is challenging, especially if they are impassable. Hence, we rely heavily on preprocedural imaging. Both computed tomography enterography (CTE) and magnetic resonance enterography (MRE) with contrast are acceptable preprocedural imaging techniques. These give us an idea of the length, number, severity, type of stricture (inflammatory versus fibrotic), presence of prestenotic dilation, and any associated fistula or abscess. All these details help us plan the procedure. Strictures longer than 5–7 cm or with significant prestenotic dilation (>5 cm in the small bowel) tend to be less responsive to EBD treatment. Avoid EBD in patients with an associated fistula or abscess. If there is a lot of inflammation on imaging, optimize medical therapy before performing an EBD.</p><p>Although there are not many scenarios where EBD is contraindicated, I recommend not performing it if there is an associated abscess or fistula with the stricture, as this may worsen the situation. Avoid EBD in patients with deep ulcerations, as these can easily cause perforation. For strictures longer than 5–6 cm, EBD may still be performed, but inform the patient of the limited success of endotherapy in such cases. EBD, in these cases of longer strictures, may serve as a bridge to surgery.</p><p>There are no clear guidelines on dilating asymptomatic strictures, making it a controversial issue. In my practice, I obtain preprocedural consent for EBD from patients with IBD. I dilate strictures even if patients are not symptomatic for several reasons. First, symptom correlation with stricture-related disease activity may not always align in CD patients; a significant stricture may present with minimal symptoms. EBD could help defer or prevent the development of symptomatic strictures. Additionally, incidentally identified strictures can impact the severity of future disease courses in IBD patients, including the development of partial small-bowel obstruction, fistula formation, and abscess formation.</p><p>EBD is a safe and efficacious endoscopic option for managing primary and anastomotic strictures. It aims to relieve obstructive symptoms and delay or avoid surgery. Patient selection and procedural planning are important to ensure this technique's success for our patients' benefit.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 8","pages":"961-964"},"PeriodicalIF":5.0000,"publicationDate":"2024-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14902","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14902","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Gursimran S. Kochhar, MD, is a gastroenterologist, Division Chief of the Department of Gastroenterology and Hepatology, at Allegheny Health Network, Pittsburgh, Pennsylvania. He specializes in interventional inflammatory bowel disease (IBD) and advanced therapeutic procedures.
Dr. Kochhar completed his training in internal medicine at Cleveland Clinic Foundation, Cleveland, Ohio, where he subsequently received training in nutrition and finished a gastroenterology and hepatology fellowship focused on training in IBD. Dr. Kochhar then completed his advanced endoscopy fellowship at Mayo Clinic, Jacksonville, Florida.
Dr. Kochhar has been at the forefront of managing IBD and its complications with various advanced endoscopic procedures. His innovative research on the endoscopic management of IBD has been successfully published in leading gastroenterology journals, including Gastroenterology, Clinical Gastroenterology and Hepatology, and Gastrointestinal Endoscopy. He has more than 120 publications, including peer-reviewed articles and book chapters. He serves on the Editorial Board of the journal Inflammatory Bowel Diseases. His current research focuses on endoscopic management of IBD complications, artificial intelligence in health care, and newer endoscopic innovations.
Stricture formation is a common complication in Crohn's disease (CD) patients, resulting from the underlying disease process, surgical anastomosis, or strictureplasty. The true incidence of stricturing disease is hard to assess. However, some studies suggest the prevalence of strictures is up to 25% in patients with CD, and over 50% of patients with CD will need at least one surgery in their lifetime.
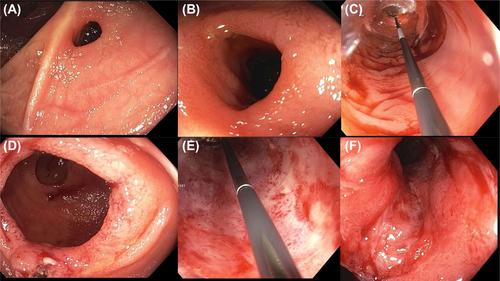
Endoscopic balloon dilation (EBD), first described by Dr. G.M. Heller in 1988 in a patient with CD,1 is a very important tool in our toolbox to manage strictures in such patients. EBD, if done well, can be very effective in mitigating or delaying surgeries in patients with CD (Fig. 1).
Endoscopic assessment of strictures is challenging, especially if they are impassable. Hence, we rely heavily on preprocedural imaging. Both computed tomography enterography (CTE) and magnetic resonance enterography (MRE) with contrast are acceptable preprocedural imaging techniques. These give us an idea of the length, number, severity, type of stricture (inflammatory versus fibrotic), presence of prestenotic dilation, and any associated fistula or abscess. All these details help us plan the procedure. Strictures longer than 5–7 cm or with significant prestenotic dilation (>5 cm in the small bowel) tend to be less responsive to EBD treatment. Avoid EBD in patients with an associated fistula or abscess. If there is a lot of inflammation on imaging, optimize medical therapy before performing an EBD.
Although there are not many scenarios where EBD is contraindicated, I recommend not performing it if there is an associated abscess or fistula with the stricture, as this may worsen the situation. Avoid EBD in patients with deep ulcerations, as these can easily cause perforation. For strictures longer than 5–6 cm, EBD may still be performed, but inform the patient of the limited success of endotherapy in such cases. EBD, in these cases of longer strictures, may serve as a bridge to surgery.
There are no clear guidelines on dilating asymptomatic strictures, making it a controversial issue. In my practice, I obtain preprocedural consent for EBD from patients with IBD. I dilate strictures even if patients are not symptomatic for several reasons. First, symptom correlation with stricture-related disease activity may not always align in CD patients; a significant stricture may present with minimal symptoms. EBD could help defer or prevent the development of symptomatic strictures. Additionally, incidentally identified strictures can impact the severity of future disease courses in IBD patients, including the development of partial small-bowel obstruction, fistula formation, and abscess formation.
EBD is a safe and efficacious endoscopic option for managing primary and anastomotic strictures. It aims to relieve obstructive symptoms and delay or avoid surgery. Patient selection and procedural planning are important to ensure this technique's success for our patients' benefit.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


