Outcomes and Survival for Early-Stage Non-Small Cell Lung Cancer Following Wedge Resection or Lobectomy: A Propensity Score-Matched Analysis Using a Novel Peruvian Registry.
Wildor Samir Cubas Llalle, Franco Albán-Sánchez, José Torres-Neyra, Wildor Dongo-Minaya, Katherine Inga-Moya, Johnny Mayta, Juan Velásquez, Jorge Mantilla, Karen Mendoza, Rafael Vicuña, Victor Mendizabal
{"title":"Outcomes and Survival for Early-Stage Non-Small Cell Lung Cancer Following Wedge Resection or Lobectomy: A Propensity Score-Matched Analysis Using a Novel Peruvian Registry.","authors":"Wildor Samir Cubas Llalle, Franco Albán-Sánchez, José Torres-Neyra, Wildor Dongo-Minaya, Katherine Inga-Moya, Johnny Mayta, Juan Velásquez, Jorge Mantilla, Karen Mendoza, Rafael Vicuña, Victor Mendizabal","doi":"10.5090/jcs.24.029","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Using a previously unreported Peruvian registry of patients treated for early-stage non-small cell lung cancer (NSCLC), this study explored whether wedge resection and lobectomy were equivalent regarding survival and impact on radiologic-pathologic variables.</p><p><strong>Methods: </strong>This observational, analytical, longitudinal study used propensity score-matched (PSM) analysis of a single-center retrospective registry of 2,570 patients with pathologic stage I-II NSCLC who were treated with wedge resection (n=1,845) or lobectomy (n=725) during 2000-2020. After PSM, 650 cases were analyzed (resection, n=325; lobectomy, n=325) through preoperative and clinical variables, including patients with ≥1 lymph node removed. Kaplan-Meier curves and multivariable Cox proportional hazard models were created for 5-year overall survival (OS), disease-free survival (DFS), and locoregional-recurrence-free survival (LRFS).</p><p><strong>Results: </strong>The principal complication was operative pain persisting >7 days for lobectomy versus wedge resection (58% vs. 23%, p=0.034) and shorter hospital stays for resection than for lobectomy (5.3 days vs. 12.8 days, p=0.009). The 5-year OS (84.3% vs. 81.2%, p=0.09) and DFS (79.1% vs. 74.1%, p=0.07) were similar and statistically insignificant between resections and lobectomies, respectively. LRFS was worse overall following wedge resection than lobectomy (79.8% vs. 91.1%, p<0.02). Nevertheless, in the PSM analysis, both groups experienced similar LRFS when the resection margin was >10 mm (90.9% vs. 87.3%, p<0.048) and ≥4 lymph nodes were removed (82.8% vs. 79.1%, p<0.011).</p><p><strong>Conclusion: </strong>Both techniques led to similar OS and DFS at 5 years; however, successful LRFS required a wedge resection with a surgical margin and adequate lymph node removal to obtain outcomes similar to lobectomy.</p>","PeriodicalId":34499,"journal":{"name":"Journal of Chest Surgery","volume":" ","pages":"501-510"},"PeriodicalIF":1.0000,"publicationDate":"2024-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11538587/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Chest Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/jcs.24.029","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/8 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Using a previously unreported Peruvian registry of patients treated for early-stage non-small cell lung cancer (NSCLC), this study explored whether wedge resection and lobectomy were equivalent regarding survival and impact on radiologic-pathologic variables.
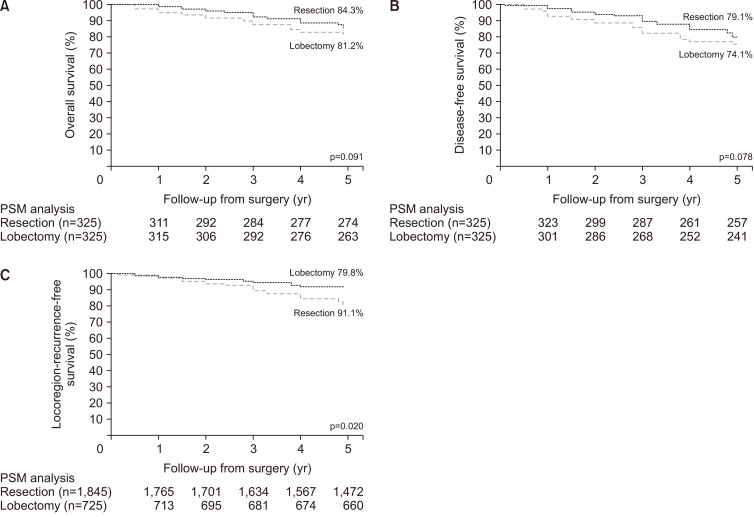
Methods: This observational, analytical, longitudinal study used propensity score-matched (PSM) analysis of a single-center retrospective registry of 2,570 patients with pathologic stage I-II NSCLC who were treated with wedge resection (n=1,845) or lobectomy (n=725) during 2000-2020. After PSM, 650 cases were analyzed (resection, n=325; lobectomy, n=325) through preoperative and clinical variables, including patients with ≥1 lymph node removed. Kaplan-Meier curves and multivariable Cox proportional hazard models were created for 5-year overall survival (OS), disease-free survival (DFS), and locoregional-recurrence-free survival (LRFS).
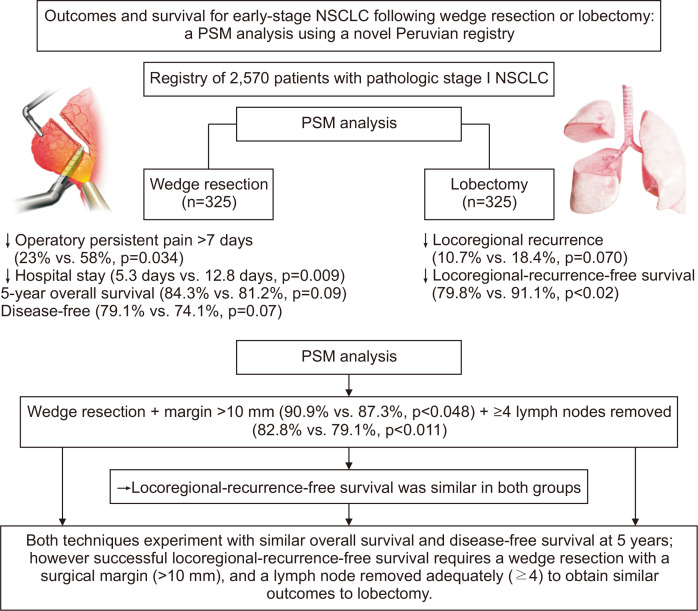
Results: The principal complication was operative pain persisting >7 days for lobectomy versus wedge resection (58% vs. 23%, p=0.034) and shorter hospital stays for resection than for lobectomy (5.3 days vs. 12.8 days, p=0.009). The 5-year OS (84.3% vs. 81.2%, p=0.09) and DFS (79.1% vs. 74.1%, p=0.07) were similar and statistically insignificant between resections and lobectomies, respectively. LRFS was worse overall following wedge resection than lobectomy (79.8% vs. 91.1%, p<0.02). Nevertheless, in the PSM analysis, both groups experienced similar LRFS when the resection margin was >10 mm (90.9% vs. 87.3%, p<0.048) and ≥4 lymph nodes were removed (82.8% vs. 79.1%, p<0.011).
Conclusion: Both techniques led to similar OS and DFS at 5 years; however, successful LRFS required a wedge resection with a surgical margin and adequate lymph node removal to obtain outcomes similar to lobectomy.
背景:本研究利用此前未报道过的秘鲁早期非小细胞肺癌(NSCLC)患者登记资料,探讨了楔形切除术和肺叶切除术在生存率和对放射病理变量的影响方面是否相同:这项观察性、分析性、纵向研究采用倾向评分匹配(PSM)分析法,对2000-2020年间接受楔形切除术(1845例)或肺叶切除术(725例)治疗的2570例病理分期为I-II期的NSCLC患者进行单中心回顾性登记。PSM 后,通过术前和临床变量分析了 650 例患者(切除术,n=325;肺叶切除术,n=325),包括切除≥1 个淋巴结的患者。建立了5年总生存期(OS)、无病生存期(DFS)和无局部复发生存期(LRFS)的Kaplan-Meier曲线和多变量Cox比例危险模型:主要并发症是肺叶切除术与楔形切除术相比,手术疼痛持续7天以上(58%对23%,P=0.034),切除术的住院时间比肺叶切除术短(5.3天对12.8天,P=0.009)。切除术和肺叶切除术的5年OS(84.3% vs. 81.2%,p=0.09)和DFS(79.1% vs. 74.1%,p=0.07)分别相似,且无统计学意义。楔形切除术的总体LRFS比肺叶切除术差(79.8% vs. 91.1%,p10 mm(90.9% vs. 87.3%,p结论:两种技术的5年OS和DFS结果相似;然而,成功的LRFS需要楔形切除术的手术边缘和足够的淋巴结切除,才能获得与肺叶切除术相似的结果。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


