Travis Pebror, Adam William Schmitz, Andrew Gauger, Reid Masterson, Sabah David Butty
{"title":"Large-bore Aspiration Thrombectomy with the FlowTriever System for the Treatment of Pulmonary Embolism: A Large Single-Center Retrospective Analysis.","authors":"Travis Pebror, Adam William Schmitz, Andrew Gauger, Reid Masterson, Sabah David Butty","doi":"10.1007/s00270-024-03819-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Evaluate the outcomes of patients undergoing large-bore aspiration thrombectomy for the treatment of pulmonary embolism at a large university medical center.</p><p><strong>Materials and methods: </strong>All patients treated for pulmonary embolism with the FlowTriever System (Inari Medical, Irvine, CA) between September 2019 and January 2023 were retrospectively analyzed. The primary safety and effectiveness outcomes included 7- and 30-day all-cause mortality, major bleeding, procedure-associated clinical decompensation, pulmonary vascular or cardiac injury, and pulmonary artery pressure reduction. Additional outcomes included technical success (completing thrombectomy with the device as intended), changes in hemodynamics and supplemental oxygen requirements, and postprocedural intensive care unit stay.</p><p><strong>Results: </strong>A total of 286 patients were identified. The mean age was 60.5 years, and 90.9% of patients presented with intermediate-risk pulmonary embolism. Technical success was achieved in 96.9% (n = 277) of cases. The average reduction in mean pulmonary arterial pressure was 6.8 mmHg, from 28.7 ± 9.0 to 21.9 ± 8.0 mmHg (p < 0.0001). Two major bleeds (0.7%), 2 pulmonary vascular injuries (0.7%), and 4 (1.4%) procedure-associated decompensations were reported, but no device-related deaths occurred. The mean post-procedure intensive care unit stay was 2.0 ± 4.1 days, and 49.3% of patients had no postprocedural intensive care unit admittance. The overall 7-day and 30-day all-cause mortality rates were 2.4% and 6.7%, respectively, with a 30-day pulmonary embolism-related mortality rate of 3.5%.</p><p><strong>Conclusion: </strong>This non-industry-sponsored single-center analysis of large-bore aspiration thrombectomy in a large population corroborates the findings of other studies and confirms that this approach is safe and effective for the treatment high- and intermediate-risk pulmonary embolism.</p><p><strong>Level of evidence iv: </strong>Retrospective observational study.</p>","PeriodicalId":9591,"journal":{"name":"CardioVascular and Interventional Radiology","volume":null,"pages":null},"PeriodicalIF":2.8000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11379772/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CardioVascular and Interventional Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00270-024-03819-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Evaluate the outcomes of patients undergoing large-bore aspiration thrombectomy for the treatment of pulmonary embolism at a large university medical center.
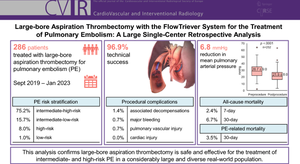
Materials and methods: All patients treated for pulmonary embolism with the FlowTriever System (Inari Medical, Irvine, CA) between September 2019 and January 2023 were retrospectively analyzed. The primary safety and effectiveness outcomes included 7- and 30-day all-cause mortality, major bleeding, procedure-associated clinical decompensation, pulmonary vascular or cardiac injury, and pulmonary artery pressure reduction. Additional outcomes included technical success (completing thrombectomy with the device as intended), changes in hemodynamics and supplemental oxygen requirements, and postprocedural intensive care unit stay.
Results: A total of 286 patients were identified. The mean age was 60.5 years, and 90.9% of patients presented with intermediate-risk pulmonary embolism. Technical success was achieved in 96.9% (n = 277) of cases. The average reduction in mean pulmonary arterial pressure was 6.8 mmHg, from 28.7 ± 9.0 to 21.9 ± 8.0 mmHg (p < 0.0001). Two major bleeds (0.7%), 2 pulmonary vascular injuries (0.7%), and 4 (1.4%) procedure-associated decompensations were reported, but no device-related deaths occurred. The mean post-procedure intensive care unit stay was 2.0 ± 4.1 days, and 49.3% of patients had no postprocedural intensive care unit admittance. The overall 7-day and 30-day all-cause mortality rates were 2.4% and 6.7%, respectively, with a 30-day pulmonary embolism-related mortality rate of 3.5%.
Conclusion: This non-industry-sponsored single-center analysis of large-bore aspiration thrombectomy in a large population corroborates the findings of other studies and confirms that this approach is safe and effective for the treatment high- and intermediate-risk pulmonary embolism.
Level of evidence iv: Retrospective observational study.
期刊介绍:
CardioVascular and Interventional Radiology (CVIR) is the official journal of the Cardiovascular and Interventional Radiological Society of Europe, and is also the official organ of a number of additional distinguished national and international interventional radiological societies. CVIR publishes double blinded peer-reviewed original research work including clinical and laboratory investigations, technical notes, case reports, works in progress, and letters to the editor, as well as review articles, pictorial essays, editorials, and special invited submissions in the field of vascular and interventional radiology. Beside the communication of the latest research results in this field, it is also the aim of CVIR to support continuous medical education. Articles that are accepted for publication are done so with the understanding that they, or their substantive contents, have not been and will not be submitted to any other publication.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


