Immediate puncture of a dislocated partially covered self-expandable metal stent in endoscopic ultrasound-guided hepaticogastrostomy for prevention of bile leakage
{"title":"Immediate puncture of a dislocated partially covered self-expandable metal stent in endoscopic ultrasound-guided hepaticogastrostomy for prevention of bile leakage","authors":"Saburo Matsubara, Kentaro Suda, Sumiko Nagoshi","doi":"10.1111/den.14903","DOIUrl":null,"url":null,"abstract":"<p>A 69-year-old woman with complex hilar strictures due to unresectable gallbladder cancer was admitted for plastic stents obstruction. Considering duodenal invasion, conversion to endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) with bridging stenting after temporary naso-biliary drainage was planned.<span><sup>1</sup></span> After puncturing B2 with a 19 G needle (Fig. 1a), two 0.025 inch guidewires were inserted into B8 and B6 using a double-lumen catheter. Two uncovered self-expandable metal stents (SEMS) were placed in both branches in partially stent-in-stent configuration. Finally, an 8 mm × 12 cm partially covered SEMS (Spring Stopper; Taewoong Medical, Seoul, Korea) with a 15 mm uncovered portion at the distal end was placed in B2 as a transluminal drainage/anastomosis stent (T-DAS). However, the T-DAS was accidentally moved toward the stomach because the tip of the inner catheter was stuck during removal.<span><sup>2</sup></span> Since the uncovered portion was suspected to be exposed to the abdominal cavity (Fig. 1b), there was concern for persistent bile leakage. Coaxial insertion of a fully-covered SEMS (HANAROSTENT Benefit; M.I.Tech, Seoul, Korea) to seal the uncovered portion failed and the guidewire was dislodged. The T-DAS within the liver parenchyma was then punctured with the 19 G needle (Fig. 1c), followed by manipulation of the 0.025 inch guidewire to bring it out of the distal end of the T-DAS into the bile duct (Fig. 1d). The HANAROSTENT Benefit was successfully placed as a second T-DAS after passing through the mesh of the first T-DAS and stopped bile leakage by completely covering the uncovered portion of the first T-DAS in the bile duct (Fig. 2, Video S1). Although computed tomography on the next day showed fluoroscopic markers at the end of the uncovered portion of the first T-DAS were outside of the liver, the clinical course was uneventful. For dislocation of a partially covered SEMS in EUS-HGS, this rescue method could be useful when coaxial fully covered SEMS insertion fails.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 11","pages":"1286-1287"},"PeriodicalIF":5.0000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14903","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14903","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
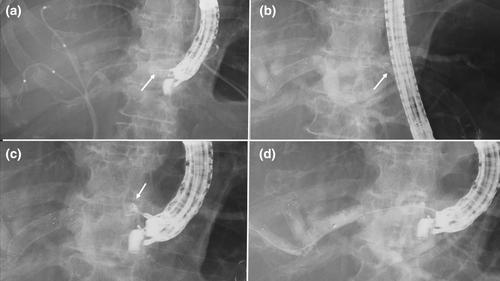
A 69-year-old woman with complex hilar strictures due to unresectable gallbladder cancer was admitted for plastic stents obstruction. Considering duodenal invasion, conversion to endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) with bridging stenting after temporary naso-biliary drainage was planned.1 After puncturing B2 with a 19 G needle (Fig. 1a), two 0.025 inch guidewires were inserted into B8 and B6 using a double-lumen catheter. Two uncovered self-expandable metal stents (SEMS) were placed in both branches in partially stent-in-stent configuration. Finally, an 8 mm × 12 cm partially covered SEMS (Spring Stopper; Taewoong Medical, Seoul, Korea) with a 15 mm uncovered portion at the distal end was placed in B2 as a transluminal drainage/anastomosis stent (T-DAS). However, the T-DAS was accidentally moved toward the stomach because the tip of the inner catheter was stuck during removal.2 Since the uncovered portion was suspected to be exposed to the abdominal cavity (Fig. 1b), there was concern for persistent bile leakage. Coaxial insertion of a fully-covered SEMS (HANAROSTENT Benefit; M.I.Tech, Seoul, Korea) to seal the uncovered portion failed and the guidewire was dislodged. The T-DAS within the liver parenchyma was then punctured with the 19 G needle (Fig. 1c), followed by manipulation of the 0.025 inch guidewire to bring it out of the distal end of the T-DAS into the bile duct (Fig. 1d). The HANAROSTENT Benefit was successfully placed as a second T-DAS after passing through the mesh of the first T-DAS and stopped bile leakage by completely covering the uncovered portion of the first T-DAS in the bile duct (Fig. 2, Video S1). Although computed tomography on the next day showed fluoroscopic markers at the end of the uncovered portion of the first T-DAS were outside of the liver, the clinical course was uneventful. For dislocation of a partially covered SEMS in EUS-HGS, this rescue method could be useful when coaxial fully covered SEMS insertion fails.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


