{"title":"Woman with fever and epigastric pain","authors":"Ping-Shih Chen MD, Kuo-Chih Chen MD, Chee-Fah Chong MS, MD","doi":"10.1002/emp2.13246","DOIUrl":null,"url":null,"abstract":"<p>A 54-year-old female without a medical history presented to the emergency department (ED) with fever and epigastric pain for 2 days. Laboratory findings showed a white blood cell count of 18,400/µL and a C-reactive protein level of 20.47 mg/dL (normal <0.5 mg/dL). Point-of-care ultrasound (POCUS) demonstrated a hypoechoic focus in the left hepatic lobe adjacent to the gastric antrum. Furthermore, a hyperechoic and linear structure, measuring 3.57 cm in length was identified, connecting those two structures (Figure 1; Video 1).</p><p>Abdominal computed tomography (CT) was performed and confirmed the diagnosis (Figure 2). Exploratory laparotomy revealed perforation of the stomach (pre-pyloric) with the fishbone penetrating the liver, which was then removed surgically (Figure 3). The patient recovered well without any complications.</p><p>Although rare, liver abscesses caused by ingested fishbones can occur. CT scans are the current diagnostic standard for such cases.<span><sup>1</sup></span> To the best of our knowledge, this is the first reported case in the English literature where POCUS has been utilized to diagnose a liver abscess caused by a fish bone. Using POCUS to determine if a liver abscess is caused by a foreign body is crucial, since its treatment often requires surgery,<span><sup>2</sup></span> as demonstrated in this case.</p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":null,"pages":null},"PeriodicalIF":1.6000,"publicationDate":"2024-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11289672/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13246","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
A 54-year-old female without a medical history presented to the emergency department (ED) with fever and epigastric pain for 2 days. Laboratory findings showed a white blood cell count of 18,400/µL and a C-reactive protein level of 20.47 mg/dL (normal <0.5 mg/dL). Point-of-care ultrasound (POCUS) demonstrated a hypoechoic focus in the left hepatic lobe adjacent to the gastric antrum. Furthermore, a hyperechoic and linear structure, measuring 3.57 cm in length was identified, connecting those two structures (Figure 1; Video 1).
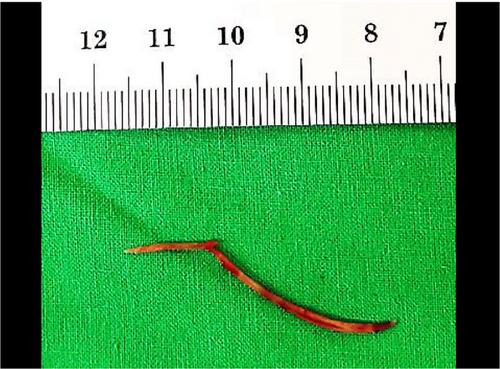
Abdominal computed tomography (CT) was performed and confirmed the diagnosis (Figure 2). Exploratory laparotomy revealed perforation of the stomach (pre-pyloric) with the fishbone penetrating the liver, which was then removed surgically (Figure 3). The patient recovered well without any complications.
Although rare, liver abscesses caused by ingested fishbones can occur. CT scans are the current diagnostic standard for such cases.1 To the best of our knowledge, this is the first reported case in the English literature where POCUS has been utilized to diagnose a liver abscess caused by a fish bone. Using POCUS to determine if a liver abscess is caused by a foreign body is crucial, since its treatment often requires surgery,2 as demonstrated in this case.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


