{"title":"Disease-burden-adapted immunotherapy protocol for primary refractory or high-risk relapsed pediatric acute lymphoblastic leukemia","authors":"Sanaa Khan, Krishnan VP, Yamini Krishnan, Gazel Sainulabdin, Somdipa Pal, Rincy Mathews, Darshan Kataria, Kunal Sehgal, Purva Kanvinde, Lashkari Harshaprasad, Minnie Bodhanwala, Bharat Agarwal, Ambreen Pandrowala, Prashant Hiwarkar","doi":"10.1002/hem3.111","DOIUrl":null,"url":null,"abstract":"<p>The survival rates for pediatric patients with primary refractory or high-risk relapsed B-cell acute lymphoblastic leukemia (r/r B-ALL), treated with chemotherapy-based protocols and followed by allogeneic hematopoietic cell transplantation (HCT), range from 15% to 30%.<span><sup>1</sup></span> These outcomes are even more unfavorable in countries with evolving healthcare insurance systems due to treatment-related mortality and financial toxicity.<span><sup>2</sup></span> The long-term event-free survival for such high-risk relapse of B-ALL is dependent on achieving minimal residual disease (MRD) negativity prior to HCT.<span><sup>3</sup></span></p><p>In the past decade, there have been significant advancements in targeted antibody-based immunotherapies for managing r/r B-ALL.<span><sup>4-11</sup></span> Blinatumomab (Blina) is a T-cell engager that provides an antileukemic effect by targeting cytotoxic T cells to CD19-expressing cancer cells. Several studies have revealed the excellent efficacy of Blina in low-burden disease.<span><sup>4-8</sup></span> However, recipients of Blina with high tumor burden have low response rates and are at risk of severe cytokine release syndrome (CRS).<span><sup>9</sup></span> Whereas, Inotuzumab ozogamicin (InO) targets CD22, which is conjugated to calicheamicin, a potent cytotoxic agent and works well even for high-burden disease with response rates as high as 80%.<span><sup>10, 11</sup></span></p><p>To optimize the use of these novel immunotherapies in r/r B-cell ALL, we designed a disease-burden-adapted protocol of InO followed by Blina for high-burden (minimal residual disease (MRD) > 5%) CD22+ CD19+ disease and Blina only for low-burden (MRD ≤ 5%) CD19+ disease.</p><p>This is a retrospective analysis of 39 patients with r/r B-cell ALL patients aged 1–18 years treated in three centers from January 2018 to August 2023. Patients were treated with a chemotherapy-based protocol from January 2018 to April 2021 and on a disease-burden-adapted immunotherapy protocol from May 2021 to August 2023.</p><p>End-of-induction (EOI) MRD of >5% with high-risk cytogenetics or age >16 years and all patients with end-of-consolidation (EOC) MRD > 0.1% irrespective of age or cytogenetics were considered primary refractory. Very early relapse (<18 months from diagnosis; marrow or isolated extramedullary), early relapse (18–36 months from diagnosis or until 6 months off therapy; marrow or isolated extramedullary), and late relapse (≥36 months from diagnosis or >6 months off therapy; marrow or isolated extramedullary) with postrelapse induction MRD of ≥0.1% and second relapse with any level of disease were considered as high-risk.</p><p>A fractionated dose of InO as 1.8 mg/m<sup>2</sup> per course was administered intravenously over 1 h on Days 1, 8, and 15 of 28-day cycle as previously described.<span><sup>10, 11</sup></span> Blina was given as a 28-day continuous intravenous infusion. The first 7 days of the first cycle were administered at 5 mcg/m<sup>2</sup>/day, and subsequently, the dose was increased to the maximum tolerated dose, up to a maximum of 15 mcg/m<sup>2</sup>/day.</p><p>Flow cytometric immunophenotypic analysis of the bone marrow was done on CD45/side scatter plots for diagnosis and follow-up MRD. In view of Blina and InO therapy, previously described alternate gating strategies were used.<span><sup>12</sup></span> Bone marrow MRD assessments were conducted after each course of immunotherapy and after HCT at 1-, 2-, 3-, 6-, and 12-month intervals.</p><p>Treatment responses were classified as complete response if MRD was negative, good response if MRD was detectable to less than 0.01%, partial response if the disease burden reduced but was more than 0.01%, and no response or progressive disease depending on whether the disease burden was stable or progressive. Patients were followed up in the clinic until November 2023.</p><p>Adverse events including neurotoxicity, cytokine release syndrome, veno-occlusive disease (VOD), and tumor lysis syndrome were graded using the CTCAE, version 5.</p><p>Overall survival was measured as time from immunotherapy to death, and event-free survival was measured as time from immunotherapy to relapse or death. We also compared the overall survival of high-risk relapsed leukemia patients in the cohort who received immunotherapy with that of high-risk relapsed leukemia patients from January 2018 to April 2021, predating the immunotherapy protocol. The Kaplan–Meier method was used to generate survival curves.</p><p>This analysis was performed in line with the principles of the Declaration of Helsinki. Bai Jerbai Wadia Hospital Ethics Committee approved retrospective analysis (Ethics No. IEC/BJWHC/AP/2024/025).</p><p>Nineteen consecutive patients with r/r B-cell ALL were treated with the disease-burden-adapted immunotherapy protocol from May 2021 to August 2023. All patients were consented for immunotherapy. The median age of the cohort was 12 years (range: 2–17 years), and two-thirds of patients were ≥10 years of age. Five were females and 14 were males. Seven patients had high-risk cytogenetics (three low hypodiploidy and one each of ABL1, iAMP21, IKZF1 deletion, and MLL-rearrangement). The demographic, leukemia characteristics, and treatment details of patients are shown in Table 1.</p><p>Eight patients were primary refractory (4 = induction failure, 4 = consolidation failure). All primary refractory patients were referred from different hospitals across the country.</p><p>Eleven patients had high-risk relapsed leukemia (2 = very early, 4 = early relapse, 2 = late relapse with post-relapse induction MRD of ≥0.1%, 3 = second relapse). Patients with relapsed leukemia received either three previous chemotherapy protocols (<i>n</i> = 5), two previous chemotherapy protocols (<i>n</i> = 5), or one previous chemotherapy protocol (<i>n</i> = 1). Ten patients received chemotherapy-based relapse induction for the latest relapse, and all had postinduction residual disease.</p><p>Five of 19 patients (26%) had an extramedullary disease, three were central nervous system positive, and two had testicular involvement.</p><p>Twelve patients (5 = primary refractory; 7 = relapsed) with MRD ranging from 0.008% to 4.21% received Blina alone (Figure 1A). The median number of Blina cycles was 2 (range: 1–3). All 12 patients achieved MRD-negative remission after the first cycle.</p><p>Seven patients (3 = primary refractory; 4 = relapsed) with high-burden disease ranging from 5.34% to 78% received one cycle of InO (Figure 1A). Six patients responded to InO; three patients became MRD-negative, and three patients achieved a good response. All six patients received consolidation with Blina and achieved MRD-negative status. One patient progressed on InO and, as a result, received palliative care.</p><p>Eighteen patients (95%) achieved MRD-negative status with the disease-burden-adapted protocol. Sixteen patients (84%) have undergone allogeneic HCT. Seven patients received grafts from haploidentical donors, six underwent matched unrelated donor HCT, and three received HCT from matched sibling donors. One patient, lacking an HLA-matched donor, underwent an autologous transplant due to high-risk pretransplant factors, such as chronic parvoviremia, intestinal adenovirus shedding, and obesity. Another patient, also without an HLA-matched donor, chose maintenance chemotherapy because of chronic parvoviremia and intestinal adenovirus shedding. Fifteen patients (77%; 95% CI: 49.5–90.6) were alive and in continuous MRD-negative CR with a median postimmunotherapy follow-up of 424 days (range: 117–914; Figure 1B,C).</p><p>Nine (82%) of 11 patients who received disease-burden-adapted protocol for relapsed leukemia were disease-free at a median follow-up of 317 days (range: 117–853). In contrast, one of 20 patients (5%) were disease-free in the preimmunotherapy high-risk relapsed leukemia cohort with a median survival of 93 days (Figure 1D; <i>p</i> < 0.0001). The comparison of the preimmunotherapy cohort versus the cohort treated with disease-burden-adapted protocol is shown in Supporting Information S1: Figure 1.</p><p>Nine (50%) patients developed mild CRS with Blina (7 = grade 1, 2 = grade 2). Two (12%) patients experienced grade 1 neurotoxicity that recovered after transient discontinuation of Blina. One patient treated with InO had grade 1 CRS. Six patients who received InO have undergone HCT to date and only one experienced mild VOD during HCT, which responded to fluid restriction and diuretics. No patients experienced immunotherapy-related grade 3 or grade 4 toxicity.</p><p>There were four deaths in the immunotherapy cohort. The causes of death included disease progression on InO in one patient, post-HCT CD19-negative relapse in another patient, and the other two patients succumbed to transplant-related mortality; one died of acute respiratory distress syndrome and another patient succumbed to early disseminated adenoviremia.</p><p>Patients diagnosed with refractory ALL inherently exhibit resistance to chemotherapy and those with relapsed ALL acquire resistance during chemotherapy exposure.<span><sup>13</sup></span> The alternative mechanism of targeting B-cell antigens with antibody-based immunotherapies provides greater opportunities for precision medicine. Clinical trials have shown that using Blina as a bridging regimen before HCT for relapsed B-cell ALL can improve disease-free survival rates.<span><sup>4-8</sup></span> At a median follow-up of 2 years, the disease-free survival rates for patients who received Blina ranged from 55% to 65%.<span><sup>4, 8</sup></span> The observations that Blina works better in the MRD setting than in hematological remission, and up to 80% of patients with high tumor burden respond to InO, formed the basis of the protocol.<span><sup>4-11</sup></span> Notably, no serious side effects were observed in this protocol. Our protocol of consolidating InO response with Blina may also reduce the risk of VOD by allowing more time between InO administration and transplant. Furthermore, exclusive use of Blina in low-burden disease could have abrogated the risk of severe CRS or neurotoxicity.</p><p>In parallel to the development of antibody-based immunotherapies, advances in cell-based immunotherapies have occurred.<span><sup>14, 15</sup></span> Cell-based immunotherapies require significant laboratory expertise and are expensive. In addition, at least 50% of patients relapse after CAR T-cell therapies and not all CAR T-cell therapies yield similar results.<span><sup>14, 16, 17</sup></span> Allogeneic HCT as a consolidative therapy after CAR T cells offsets the potential benefits of autologous CAR T cells. In contrast, antibody-based therapies are off-the-shelf, manufacture-controlled, and do not require infrastructure, making them a more viable option in regions with emerging healthcare insurance systems.</p><p>To conclude, the disease-burden-adapted protocol is a promising strategy for treating r/r pediatric B-ALL as a bridging regimen before HCT. The report underscores the importance of making these immunotherapies accessible on a global scale through collaborative efforts involving governments, nongovernmental organizations, and pharmaceutical initiatives. While the analysis is retrospective, its findings highlight the efficacy and safety of this strategy allowing a greater number of patients to reach potentially curative HCT.</p><p>Prashant Hiwarkar conceived the study and analyzed the data. Sanaa Khan, Krishnan VP, Lashkari Harshaprasad, and Purva Kanvinde acquired the data. Sanaa Khan, Krishnan VP, and Prashant Hiwarkar wrote the manuscript. Kunal Sehgal did flow cytometry analysis. Sanaa Khan, Krishnan VP, Yamini Krishnan, Gazel Sainulabdin, Somdipa Pal, Rincy Mathews, Darshan Kataria, Minnie Bodhanwala, Bharat Agarwal, Ambreen Pandrowala, and Prashant Hiwarkar were actively involved in patient care; all authors revised and approved the final manuscript.</p><p>The authors declare no conflict of interest.</p><p>This research received no funding.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 8","pages":""},"PeriodicalIF":7.6000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11284769/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.111","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
The survival rates for pediatric patients with primary refractory or high-risk relapsed B-cell acute lymphoblastic leukemia (r/r B-ALL), treated with chemotherapy-based protocols and followed by allogeneic hematopoietic cell transplantation (HCT), range from 15% to 30%.1 These outcomes are even more unfavorable in countries with evolving healthcare insurance systems due to treatment-related mortality and financial toxicity.2 The long-term event-free survival for such high-risk relapse of B-ALL is dependent on achieving minimal residual disease (MRD) negativity prior to HCT.3
In the past decade, there have been significant advancements in targeted antibody-based immunotherapies for managing r/r B-ALL.4-11 Blinatumomab (Blina) is a T-cell engager that provides an antileukemic effect by targeting cytotoxic T cells to CD19-expressing cancer cells. Several studies have revealed the excellent efficacy of Blina in low-burden disease.4-8 However, recipients of Blina with high tumor burden have low response rates and are at risk of severe cytokine release syndrome (CRS).9 Whereas, Inotuzumab ozogamicin (InO) targets CD22, which is conjugated to calicheamicin, a potent cytotoxic agent and works well even for high-burden disease with response rates as high as 80%.10, 11
To optimize the use of these novel immunotherapies in r/r B-cell ALL, we designed a disease-burden-adapted protocol of InO followed by Blina for high-burden (minimal residual disease (MRD) > 5%) CD22+ CD19+ disease and Blina only for low-burden (MRD ≤ 5%) CD19+ disease.
This is a retrospective analysis of 39 patients with r/r B-cell ALL patients aged 1–18 years treated in three centers from January 2018 to August 2023. Patients were treated with a chemotherapy-based protocol from January 2018 to April 2021 and on a disease-burden-adapted immunotherapy protocol from May 2021 to August 2023.
End-of-induction (EOI) MRD of >5% with high-risk cytogenetics or age >16 years and all patients with end-of-consolidation (EOC) MRD > 0.1% irrespective of age or cytogenetics were considered primary refractory. Very early relapse (<18 months from diagnosis; marrow or isolated extramedullary), early relapse (18–36 months from diagnosis or until 6 months off therapy; marrow or isolated extramedullary), and late relapse (≥36 months from diagnosis or >6 months off therapy; marrow or isolated extramedullary) with postrelapse induction MRD of ≥0.1% and second relapse with any level of disease were considered as high-risk.
A fractionated dose of InO as 1.8 mg/m2 per course was administered intravenously over 1 h on Days 1, 8, and 15 of 28-day cycle as previously described.10, 11 Blina was given as a 28-day continuous intravenous infusion. The first 7 days of the first cycle were administered at 5 mcg/m2/day, and subsequently, the dose was increased to the maximum tolerated dose, up to a maximum of 15 mcg/m2/day.
Flow cytometric immunophenotypic analysis of the bone marrow was done on CD45/side scatter plots for diagnosis and follow-up MRD. In view of Blina and InO therapy, previously described alternate gating strategies were used.12 Bone marrow MRD assessments were conducted after each course of immunotherapy and after HCT at 1-, 2-, 3-, 6-, and 12-month intervals.
Treatment responses were classified as complete response if MRD was negative, good response if MRD was detectable to less than 0.01%, partial response if the disease burden reduced but was more than 0.01%, and no response or progressive disease depending on whether the disease burden was stable or progressive. Patients were followed up in the clinic until November 2023.
Adverse events including neurotoxicity, cytokine release syndrome, veno-occlusive disease (VOD), and tumor lysis syndrome were graded using the CTCAE, version 5.
Overall survival was measured as time from immunotherapy to death, and event-free survival was measured as time from immunotherapy to relapse or death. We also compared the overall survival of high-risk relapsed leukemia patients in the cohort who received immunotherapy with that of high-risk relapsed leukemia patients from January 2018 to April 2021, predating the immunotherapy protocol. The Kaplan–Meier method was used to generate survival curves.
This analysis was performed in line with the principles of the Declaration of Helsinki. Bai Jerbai Wadia Hospital Ethics Committee approved retrospective analysis (Ethics No. IEC/BJWHC/AP/2024/025).
Nineteen consecutive patients with r/r B-cell ALL were treated with the disease-burden-adapted immunotherapy protocol from May 2021 to August 2023. All patients were consented for immunotherapy. The median age of the cohort was 12 years (range: 2–17 years), and two-thirds of patients were ≥10 years of age. Five were females and 14 were males. Seven patients had high-risk cytogenetics (three low hypodiploidy and one each of ABL1, iAMP21, IKZF1 deletion, and MLL-rearrangement). The demographic, leukemia characteristics, and treatment details of patients are shown in Table 1.
Eight patients were primary refractory (4 = induction failure, 4 = consolidation failure). All primary refractory patients were referred from different hospitals across the country.
Eleven patients had high-risk relapsed leukemia (2 = very early, 4 = early relapse, 2 = late relapse with post-relapse induction MRD of ≥0.1%, 3 = second relapse). Patients with relapsed leukemia received either three previous chemotherapy protocols (n = 5), two previous chemotherapy protocols (n = 5), or one previous chemotherapy protocol (n = 1). Ten patients received chemotherapy-based relapse induction for the latest relapse, and all had postinduction residual disease.
Five of 19 patients (26%) had an extramedullary disease, three were central nervous system positive, and two had testicular involvement.
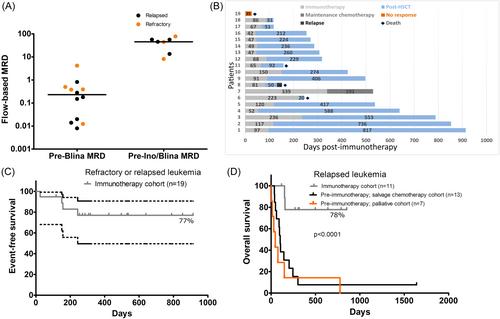
Twelve patients (5 = primary refractory; 7 = relapsed) with MRD ranging from 0.008% to 4.21% received Blina alone (Figure 1A). The median number of Blina cycles was 2 (range: 1–3). All 12 patients achieved MRD-negative remission after the first cycle.
Seven patients (3 = primary refractory; 4 = relapsed) with high-burden disease ranging from 5.34% to 78% received one cycle of InO (Figure 1A). Six patients responded to InO; three patients became MRD-negative, and three patients achieved a good response. All six patients received consolidation with Blina and achieved MRD-negative status. One patient progressed on InO and, as a result, received palliative care.
Eighteen patients (95%) achieved MRD-negative status with the disease-burden-adapted protocol. Sixteen patients (84%) have undergone allogeneic HCT. Seven patients received grafts from haploidentical donors, six underwent matched unrelated donor HCT, and three received HCT from matched sibling donors. One patient, lacking an HLA-matched donor, underwent an autologous transplant due to high-risk pretransplant factors, such as chronic parvoviremia, intestinal adenovirus shedding, and obesity. Another patient, also without an HLA-matched donor, chose maintenance chemotherapy because of chronic parvoviremia and intestinal adenovirus shedding. Fifteen patients (77%; 95% CI: 49.5–90.6) were alive and in continuous MRD-negative CR with a median postimmunotherapy follow-up of 424 days (range: 117–914; Figure 1B,C).
Nine (82%) of 11 patients who received disease-burden-adapted protocol for relapsed leukemia were disease-free at a median follow-up of 317 days (range: 117–853). In contrast, one of 20 patients (5%) were disease-free in the preimmunotherapy high-risk relapsed leukemia cohort with a median survival of 93 days (Figure 1D; p < 0.0001). The comparison of the preimmunotherapy cohort versus the cohort treated with disease-burden-adapted protocol is shown in Supporting Information S1: Figure 1.
Nine (50%) patients developed mild CRS with Blina (7 = grade 1, 2 = grade 2). Two (12%) patients experienced grade 1 neurotoxicity that recovered after transient discontinuation of Blina. One patient treated with InO had grade 1 CRS. Six patients who received InO have undergone HCT to date and only one experienced mild VOD during HCT, which responded to fluid restriction and diuretics. No patients experienced immunotherapy-related grade 3 or grade 4 toxicity.
There were four deaths in the immunotherapy cohort. The causes of death included disease progression on InO in one patient, post-HCT CD19-negative relapse in another patient, and the other two patients succumbed to transplant-related mortality; one died of acute respiratory distress syndrome and another patient succumbed to early disseminated adenoviremia.
Patients diagnosed with refractory ALL inherently exhibit resistance to chemotherapy and those with relapsed ALL acquire resistance during chemotherapy exposure.13 The alternative mechanism of targeting B-cell antigens with antibody-based immunotherapies provides greater opportunities for precision medicine. Clinical trials have shown that using Blina as a bridging regimen before HCT for relapsed B-cell ALL can improve disease-free survival rates.4-8 At a median follow-up of 2 years, the disease-free survival rates for patients who received Blina ranged from 55% to 65%.4, 8 The observations that Blina works better in the MRD setting than in hematological remission, and up to 80% of patients with high tumor burden respond to InO, formed the basis of the protocol.4-11 Notably, no serious side effects were observed in this protocol. Our protocol of consolidating InO response with Blina may also reduce the risk of VOD by allowing more time between InO administration and transplant. Furthermore, exclusive use of Blina in low-burden disease could have abrogated the risk of severe CRS or neurotoxicity.
In parallel to the development of antibody-based immunotherapies, advances in cell-based immunotherapies have occurred.14, 15 Cell-based immunotherapies require significant laboratory expertise and are expensive. In addition, at least 50% of patients relapse after CAR T-cell therapies and not all CAR T-cell therapies yield similar results.14, 16, 17 Allogeneic HCT as a consolidative therapy after CAR T cells offsets the potential benefits of autologous CAR T cells. In contrast, antibody-based therapies are off-the-shelf, manufacture-controlled, and do not require infrastructure, making them a more viable option in regions with emerging healthcare insurance systems.
To conclude, the disease-burden-adapted protocol is a promising strategy for treating r/r pediatric B-ALL as a bridging regimen before HCT. The report underscores the importance of making these immunotherapies accessible on a global scale through collaborative efforts involving governments, nongovernmental organizations, and pharmaceutical initiatives. While the analysis is retrospective, its findings highlight the efficacy and safety of this strategy allowing a greater number of patients to reach potentially curative HCT.
Prashant Hiwarkar conceived the study and analyzed the data. Sanaa Khan, Krishnan VP, Lashkari Harshaprasad, and Purva Kanvinde acquired the data. Sanaa Khan, Krishnan VP, and Prashant Hiwarkar wrote the manuscript. Kunal Sehgal did flow cytometry analysis. Sanaa Khan, Krishnan VP, Yamini Krishnan, Gazel Sainulabdin, Somdipa Pal, Rincy Mathews, Darshan Kataria, Minnie Bodhanwala, Bharat Agarwal, Ambreen Pandrowala, and Prashant Hiwarkar were actively involved in patient care; all authors revised and approved the final manuscript.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


