{"title":"Full Outline of Unresponsiveness Score versus Glasgow Coma Scale in Predicting Clinical Outcomes in Altered Mental Status.","authors":"Savan Pandey, Ankit Kumar Sahu, Meera Ekka, Priyanka Modi, Praveen Aggarwal, Nayer Jamshed, Sanjeev Bhoi","doi":"10.4103/jets.jets_76_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Full outline of unresponsiveness (FOUR) score has advantages over Glasgow Coma Scale (GCS); as it can be used in intubated patients and provides greater neurological details. It has been studied mainly in the trauma and neuroscience setting. Our primary objective was to compare the FOUR versus GCS score as predictors of mortality at 30 days and poor functional outcome at 3 months among nontrauma patients in the emergency department (ED).</p><p><strong>Methods: </strong>This prospective observational study was conducted on adult patients presenting with altered mental status (duration <7 days) in the ED (March 2019-November 2020). Data collection included demographic and clinical features, the GCS and FOUR scores, the feasibility of acquiring and interpreting FOUR on a Likert scale, duration of hospital stay, 30-day mortality, and functional outcome at 3 months on the modified Rankin Scale. Trained emergency medicine residents managing the patient collected the data. The area under receiver's operating characteristics curve (AUROC) was used to compare the accuracy of the GCS and FOUR scores in predicting outcomes. The FOUR score equivalent of GCS cutoffs for categorizing neurological impairment (mild, moderate, and severe) was also investigated.</p><p><strong>Results: </strong>Two hundred and ninety-one patients were included, with a mean age of 50.3 years and 67.4% males. Most patients (40.2%) had altered mental status for 1-3 days and hepatic encephalopathy was the most common ED diagnosis. The mortality at 30 days was 66.7% (194 of 291), and 88% (256 of 291) of patients had poor functional outcomes at 3 months. The AUROCs for predicting 30-day mortality were similar for both the scores (GCS: 0.70, FOUR: 0.71, and the <i>P</i> value for difference: 0.9). Similarly, the AUROCs for predicting 3-month poor functional outcome were 0.683 and 0.669 using GCS and FOUR, respectively, with a nonsignificant difference (<i>P</i> = 0.82). The FOUR score strata of 14-16, 11-13, and 0-10 were found to be equivalent to the GCS scores of 13-15 (mild), 9-12 (moderate), and 3-8 (severe). The feasibility of acquiring and interpreting GCS and FOUR scores on the Likert scale was found to be \"easy.\"</p><p><strong>Conclusion: </strong>The FOUR score is similar to GCS in predicting mortality at 30 days and poor neurological outcomes at 3 months among nontrauma patients of ED. Moreover, it was found that the FOUR score is \"easy\" to assess and interpret by the emergency residents.</p>","PeriodicalId":15692,"journal":{"name":"Journal of Emergencies, Trauma, and Shock","volume":"17 2","pages":"102-106"},"PeriodicalIF":0.7000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11279499/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Emergencies, Trauma, and Shock","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jets.jets_76_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Full outline of unresponsiveness (FOUR) score has advantages over Glasgow Coma Scale (GCS); as it can be used in intubated patients and provides greater neurological details. It has been studied mainly in the trauma and neuroscience setting. Our primary objective was to compare the FOUR versus GCS score as predictors of mortality at 30 days and poor functional outcome at 3 months among nontrauma patients in the emergency department (ED).
Methods: This prospective observational study was conducted on adult patients presenting with altered mental status (duration <7 days) in the ED (March 2019-November 2020). Data collection included demographic and clinical features, the GCS and FOUR scores, the feasibility of acquiring and interpreting FOUR on a Likert scale, duration of hospital stay, 30-day mortality, and functional outcome at 3 months on the modified Rankin Scale. Trained emergency medicine residents managing the patient collected the data. The area under receiver's operating characteristics curve (AUROC) was used to compare the accuracy of the GCS and FOUR scores in predicting outcomes. The FOUR score equivalent of GCS cutoffs for categorizing neurological impairment (mild, moderate, and severe) was also investigated.
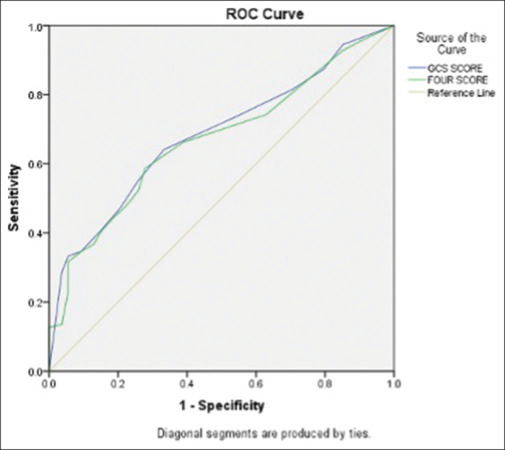
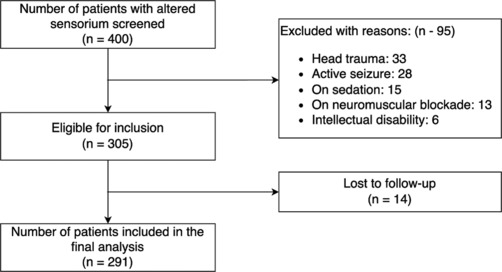
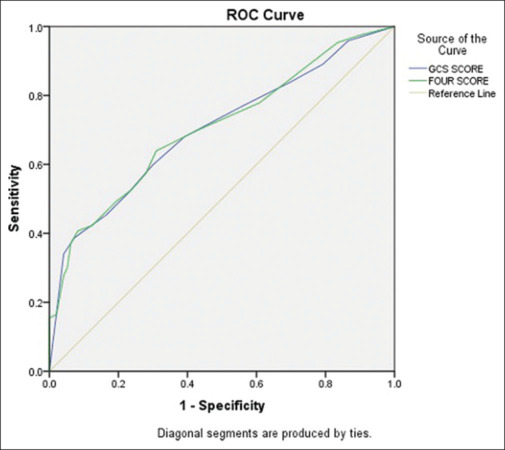
Results: Two hundred and ninety-one patients were included, with a mean age of 50.3 years and 67.4% males. Most patients (40.2%) had altered mental status for 1-3 days and hepatic encephalopathy was the most common ED diagnosis. The mortality at 30 days was 66.7% (194 of 291), and 88% (256 of 291) of patients had poor functional outcomes at 3 months. The AUROCs for predicting 30-day mortality were similar for both the scores (GCS: 0.70, FOUR: 0.71, and the P value for difference: 0.9). Similarly, the AUROCs for predicting 3-month poor functional outcome were 0.683 and 0.669 using GCS and FOUR, respectively, with a nonsignificant difference (P = 0.82). The FOUR score strata of 14-16, 11-13, and 0-10 were found to be equivalent to the GCS scores of 13-15 (mild), 9-12 (moderate), and 3-8 (severe). The feasibility of acquiring and interpreting GCS and FOUR scores on the Likert scale was found to be "easy."
Conclusion: The FOUR score is similar to GCS in predicting mortality at 30 days and poor neurological outcomes at 3 months among nontrauma patients of ED. Moreover, it was found that the FOUR score is "easy" to assess and interpret by the emergency residents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


