Clara Massaguer, Laura Saura-García, Pedro Palazón, Gastón Echaniz, Maria Carme Roqueta Alcaraz, Xavier Tarrado
{"title":"Bilateral Lung Injury with Delayed Pneumothorax following Preoperative Cryoanalgesia for Pectus Excavatum Repair in a 13-year-old Boy.","authors":"Clara Massaguer, Laura Saura-García, Pedro Palazón, Gastón Echaniz, Maria Carme Roqueta Alcaraz, Xavier Tarrado","doi":"10.1055/a-2349-9668","DOIUrl":null,"url":null,"abstract":"<p><p>A 13-year-old male patient with marfanoid features and pectus excavatum with Haller index 4 and correction index of 38% underwent the Nuss procedure with cryoanalgesia 9 days prior, which transpired uneventfully. Preoperative spirometry was normal, and echocardiogram showed light aortic valve dilation. A month later, during a routine outpatient checkup, he referred middle abdominal pain, denying respiratory symptoms nor thoracic pain. He presented bilateral apical and right basal hypophonesis. Chest X-ray revealed bilateral pneumothorax and right pleural effusion. Consequently, the patient was admitted to the emergency room, and a chest computed tomography was ordered, reporting right apical blebs. Bilateral thoracoscopy was performed, and apexes were checked for pulmonary blebs to rule out primary pneumothorax. In the right chest, a wedge resection of a distorted area on the apex and pleuroabrasion were done. Four air leaking eschars were found when performing lung expansion under water as leaking test, corresponding to cryoanalgesia intercostal eschars, and subsequently closed by primary suture. In the left chest, there were no blebs. However, another four pleural lesions with intact pleura in the left lower lobe were also found. Postoperative course was uneventful and chest drains were removed 48 hours after surgery. He remains asymptomatic 21 months after discharge. Cryoanalgesia in pectus excavatum is spreading due to the improvement in postoperative pain control. However, some complications may occur.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":"12 1","pages":"e50-e53"},"PeriodicalIF":0.7000,"publicationDate":"2024-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11281861/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2349-9668","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
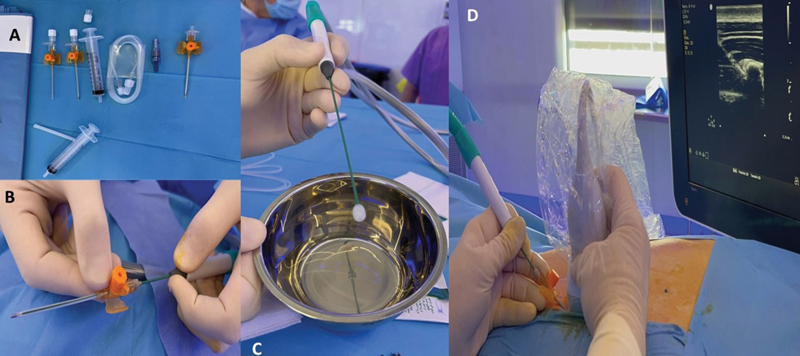
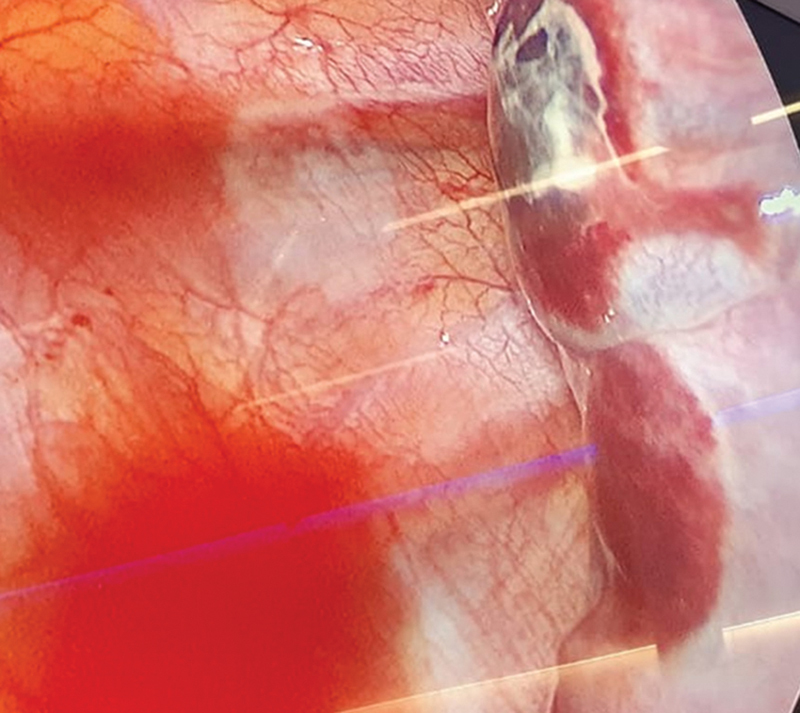
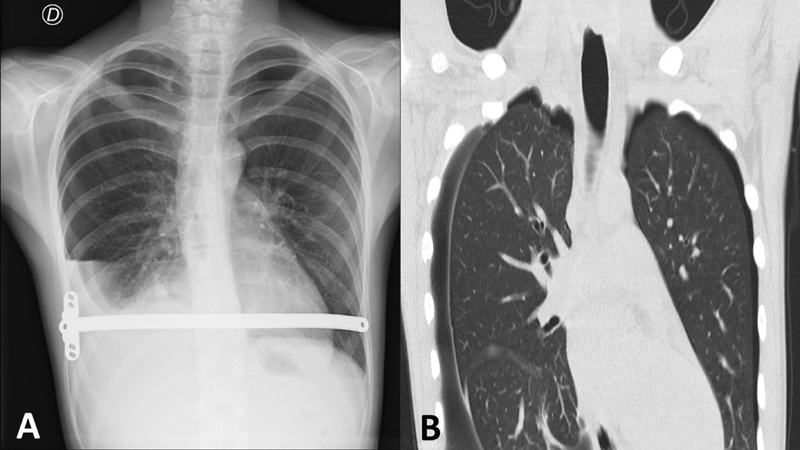
A 13-year-old male patient with marfanoid features and pectus excavatum with Haller index 4 and correction index of 38% underwent the Nuss procedure with cryoanalgesia 9 days prior, which transpired uneventfully. Preoperative spirometry was normal, and echocardiogram showed light aortic valve dilation. A month later, during a routine outpatient checkup, he referred middle abdominal pain, denying respiratory symptoms nor thoracic pain. He presented bilateral apical and right basal hypophonesis. Chest X-ray revealed bilateral pneumothorax and right pleural effusion. Consequently, the patient was admitted to the emergency room, and a chest computed tomography was ordered, reporting right apical blebs. Bilateral thoracoscopy was performed, and apexes were checked for pulmonary blebs to rule out primary pneumothorax. In the right chest, a wedge resection of a distorted area on the apex and pleuroabrasion were done. Four air leaking eschars were found when performing lung expansion under water as leaking test, corresponding to cryoanalgesia intercostal eschars, and subsequently closed by primary suture. In the left chest, there were no blebs. However, another four pleural lesions with intact pleura in the left lower lobe were also found. Postoperative course was uneventful and chest drains were removed 48 hours after surgery. He remains asymptomatic 21 months after discharge. Cryoanalgesia in pectus excavatum is spreading due to the improvement in postoperative pain control. However, some complications may occur.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


