Reinsertion of a removed self-expandable metal stent through an endosonographically created route after hepaticojejunostomy for multiple cholangioscopy-guided procedures
{"title":"Reinsertion of a removed self-expandable metal stent through an endosonographically created route after hepaticojejunostomy for multiple cholangioscopy-guided procedures","authors":"Saburo Matsubara, Kentaro Suda, Sumiko Nagoshi","doi":"10.1111/den.14899","DOIUrl":null,"url":null,"abstract":"<p>In recent years, antegrade treatment via an endosonographically created route (ESCR) for choledocholithiasis in patients with surgically altered anatomy (SAA) has emerged.<span><sup>1, 2</sup></span> A self-expandable metal stent (SEMS) can form thicker ESCR to facilitate cholangioscopy-guided electrohydraulic lithotripsy (EHL).<span><sup>3</sup></span> If repeat EHL is required, another SEMS should be placed to maintain ESCR, but at a cost. Herein, we present a method for reinserting a removed SEMS.</p><p>A 76-year-old man with a history of total gastrectomy was admitted for obstructive jaundice due to large common bile duct stones (Fig. 1a). First, endoscopic ultrasound-guided hepaticojejunostomy (EUS-HJS) was performed, using an 8 mm partially covered SEMS (Spring Stopper; Taewoong Medical, Seoul, Korea) (Fig. 1b) to prevent focal cholangitis. One week later, the stent was removed through the channel without resistance, suggesting an absence of tissue hyperplasia in the uncovered area due to the short indwelling time. Then a SpyGlass DS II (Boston Scientific, Natick, MA, USA) was inserted through the ESCR and EHL was performed. Since the stones could not be sufficiently crushed after 1 h, we decided to reinsert the stent for the next session. After attaching a looped nylon thread to the tip of the stent (Fig. 2a), a guidewire indwelling in the ESCR was inserted through the tip of the stent. A wire-guided forceps (Histoguide; STERIS, Mentor, OH, USA) (Fig. 2b) was inserted over the guidewire from the end of the stent to grasp the loop (Fig. 2c). The stent was then inserted into the channel with the lid removed, while being stretched and twisted together with the forceps. Following insertion of the stent into the bile duct, the guidewire and forceps were removed (Video S1). The stones were completely removed during the next cholangioscopy-guided EHL.</p><p>Reuse of a single SEMS with this method for multiple cholangioscopy-guided procedures via an ESCR would be cost beneficial.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 10","pages":"1183-1184"},"PeriodicalIF":5.0000,"publicationDate":"2024-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14899","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14899","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
In recent years, antegrade treatment via an endosonographically created route (ESCR) for choledocholithiasis in patients with surgically altered anatomy (SAA) has emerged.1, 2 A self-expandable metal stent (SEMS) can form thicker ESCR to facilitate cholangioscopy-guided electrohydraulic lithotripsy (EHL).3 If repeat EHL is required, another SEMS should be placed to maintain ESCR, but at a cost. Herein, we present a method for reinserting a removed SEMS.
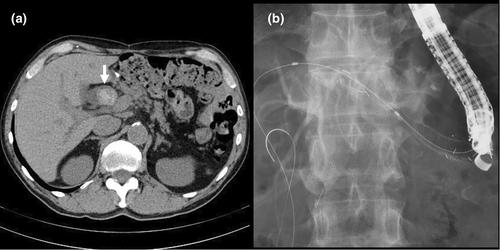
A 76-year-old man with a history of total gastrectomy was admitted for obstructive jaundice due to large common bile duct stones (Fig. 1a). First, endoscopic ultrasound-guided hepaticojejunostomy (EUS-HJS) was performed, using an 8 mm partially covered SEMS (Spring Stopper; Taewoong Medical, Seoul, Korea) (Fig. 1b) to prevent focal cholangitis. One week later, the stent was removed through the channel without resistance, suggesting an absence of tissue hyperplasia in the uncovered area due to the short indwelling time. Then a SpyGlass DS II (Boston Scientific, Natick, MA, USA) was inserted through the ESCR and EHL was performed. Since the stones could not be sufficiently crushed after 1 h, we decided to reinsert the stent for the next session. After attaching a looped nylon thread to the tip of the stent (Fig. 2a), a guidewire indwelling in the ESCR was inserted through the tip of the stent. A wire-guided forceps (Histoguide; STERIS, Mentor, OH, USA) (Fig. 2b) was inserted over the guidewire from the end of the stent to grasp the loop (Fig. 2c). The stent was then inserted into the channel with the lid removed, while being stretched and twisted together with the forceps. Following insertion of the stent into the bile duct, the guidewire and forceps were removed (Video S1). The stones were completely removed during the next cholangioscopy-guided EHL.
Reuse of a single SEMS with this method for multiple cholangioscopy-guided procedures via an ESCR would be cost beneficial.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


