Prophylactic tocilizumab reduces the incidence of cytokine release syndrome in relapsed/refractory myeloma patients treated with teclistamab: Implications for outpatient step-up dosing
Charlotte L. B. M. Korst, Kaz Groen, Patricia W. C. Bosman, Fleur van der Valk, Christie P. M. Verkleij, Sandy Kruyswijk, Maaike E. M. de Ruijter, Dianne M. Heijink, Maria T. Kuipers, Sonja Zweegman, Niels W. C. J. van de Donk
{"title":"Prophylactic tocilizumab reduces the incidence of cytokine release syndrome in relapsed/refractory myeloma patients treated with teclistamab: Implications for outpatient step-up dosing","authors":"Charlotte L. B. M. Korst, Kaz Groen, Patricia W. C. Bosman, Fleur van der Valk, Christie P. M. Verkleij, Sandy Kruyswijk, Maaike E. M. de Ruijter, Dianne M. Heijink, Maria T. Kuipers, Sonja Zweegman, Niels W. C. J. van de Donk","doi":"10.1002/hem3.132","DOIUrl":null,"url":null,"abstract":"<p>Teclistamab, a T-cell redirecting bispecific antibody (BsAb) targeting B-cell maturation antigen (BCMA), has marked activity in heavily pretreated multiple myeloma (MM) patients (overall response rate: 63.0%; at least very good partial response [≥VGPR]: 59.4%; median progression-free survival [PFS]: 11.3 months).<span><sup>1, 2</sup></span> Teclistamab treatment induces T-cell activation and production of proinflammatory cytokines such as interleukin-6 (IL-6).<span><sup>3</sup></span> This increase in cytokines frequently results in a systemic inflammatory response syndrome (cytokine-release syndrome [CRS]), characterized by fever, and in more severe cases also hypotension and hypoxia.<span><sup>1, 2, 4, 5</sup></span> CRS mitigation strategies include step-up dosing and premedication with steroids and antihistamines. The incidence of CRS in teclistamab-treated patients was 72.1% (grade 2: 21.2%; grade ≥3: 0.6%) with most CRS events occurring during step-up dosing.<span><sup>1, 2, 4</sup></span> Recurrent CRS occurred in 33.3% of the patients.<span><sup>4</sup></span> Patients are generally hospitalized for the administration of the step-up doses and first full dose to adequately monitor for early signs and symptoms of CRS (median hospital stay in a real-world setting: 10 days).<span><sup>1, 6</sup></span> Treatment of CRS with steroids or the IL-6 receptor-blocking antibody tocilizumab is effective with rapid resolution of symptoms.<span><sup>3, 4</sup></span> Patients who received tocilizumab for their first CRS event were less likely to experience a subsequent CRS event compared to those who did not receive tocilizumab (20.0% vs. 62.2%).<span><sup>4</sup></span> A single dose of tocilizumab blocks the IL-6 receptor for approximately 10 days and covers the full step-up dosing period.<span><sup>7</sup></span> Based on these data, we aimed to evaluate the efficacy of tocilizumab administered prior to the first step-up dose to prevent the development of CRS following the initiation of teclistamab therapy in 29 patients treated in our hospital.</p><p>Teclistamab was administered according to the approved schedule with two step-up doses (0.06 and 0.3 mg/kg) followed by the full dose of 1.5 mg/kg every week (48–72 h between step-up doses and the first full dose). In patients undergoing hemodialysis, teclistamab was given directly after hemodialysis sessions. Prophylactic tocilizumab (8 mg/kg intravenously [IV]; maximum dose of 800 mg) was administered 1 h prior to the first step-up dose. Patients also received 16 mg dexamethasone, 2 mg clemastine, and 1000 mg acetaminophen 1 h prior to both step-up doses and the first full dose. All patients received herpes zoster (valacyclovir) and <i>Pneumocystis jirovecii</i> pneumonia prophylaxis (co-trimoxazole, or pentamidine in case of co-trimoxazole allergy). Granulocyte colony-stimulating factor was considered in cases of grade ≥3 neutropenia, and IgG replacement was given in cases with polyclonal IgG <4 g/L (either as primary or secondary prophylaxis at individual physician's discretion). At the current follow-up, 26 patients (89.7%) received IgG replacement. Patients did not receive other antibacterial or antifungal prophylaxis. CRS and immune effector cell-associated neurotoxicity syndrome (ICANS) were graded according to the American Society for Transplantation and Cellular Therapy criteria.<span><sup>5</sup></span></p><p>Prophylactic tocilizumab was given from October 2022 to March 2024 to all relapsed/refractory MM patients who received teclistamab monotherapy as part of a compassionate use program (CUP; <i>n</i> = 20) and also to nine consecutive patients who received teclistamab in the MajesTEC-1 trial<span><sup>1</sup></span> (total number of patients: 29). The study site ethics committee approved the protocols, which were conducted according to the principles of the Declaration of Helsinki, the International Conference on Harmonization, and the Guidelines for Good Clinical Practice. All patients provided written informed consent.</p><p>Patient characteristics are shown in Table 1. Patients had received a median of four prior lines of therapy. None of the patients had prior exposure to a BCMA-directed therapy, and only one patient was previously treated with a non-BCMA-targeting BsAb (talquetamab). The majority of the CUP patients (90%) would not have met the eligibility criteria for MajesTEC-1 due to the presence of oligosecretory disease (<i>n</i> = 7), severe cytopenias (<i>n</i> = 7), renal impairment (<i>n</i> = 3, including hemodialysis in one patient), cardiac conditions (<i>n</i> = 2, one patient with heart failure [New York Heart Association class III] and one with Brugada syndrome), and/or other reasons.</p><p>CRS occurred in only three of the 29 patients (10.3%); one patient with grade 1 CRS after step-up dose 1, one patient with grade 2 CRS after step-up dose 1, and one patient with grade 1 CRS after step-up dose 2 and grade 2 CRS after the first full dose (Figure 1A). CRS treatment consisted of additional tocilizumab administration in all three patients and dexamethasone (10 mg IV) in the patient with recurrent CRS. Both patients with grade 2 CRS also received IV fluids because of hypotension. The median duration of CRS was one day (range, 1–3). All CRS events were resolved completely.</p><p>Both patients who developed grade 2 CRS despite prophylactic tocilizumab had high tumor burden (70%–80% MM cells in bone marrow [BM] biopsy) and rapidly progressive disease (light-chain doubling time of approximately 4 weeks prior to initiation of teclistamab treatment), which was not the case in the patient with grade 1 CRS (30% MM cells in BM biopsy; increase in light-chain level by 25% during the 4 weeks prior to the first teclistamab dose). Evaluation of the peripheral blood smears by conventional microscopy revealed circulating tumor cells in one of the three patients who developed CRS (patient with recurrent CRS). Circulating tumor cells were not detected in the blood smear of patients who did not develop CRS.</p><p>Twenty-five patients received teclistamab step-up dosing in the inpatient setting. The median duration of hospitalization for step-up dosing was 8 days (interquartile range, 6–9 days), with only one patient staying 2 days longer than expected because of grade 2 CRS after the first full dose. Notably, four patients received teclistamab step-up dosing in the outpatient setting with tocilizumab prophylaxis without the development of CRS or the need for hospitalization. These patients lived relatively close to the hospital (<60 min travel time) and were in the company of a competent adult.</p><p>Overall, tocilizumab prophylaxis had no negative impact on the activity of teclistamab with 24 of the 29 patients (82.8%) achieving a partial response or better with ≥VGPR in 75.9%. With a median follow-up of 8.7 months, the median PFS was not reached (12-month PFS: 63.5%). OS at 12 months was 72.2% (Figure 1B–D). All three patients with renal impairment responded, including the patient who received hemodialysis (VGPR). Except for the lower CRS rate, the safety profile of teclistamab with prophylactic tocilizumab was comparable to that observed in the MajesTEC-1 trial<span><sup>1, 2</sup></span> with grade ≥3 thrombocytopenia in 13.8%, grade ≥3 anemia in 6.9%, and grade ≥3 infections in 27.6%. ICANS, which typically concurs with CRS, was observed in none of the 29 patients. Also, the frequency and median duration of grade ≥3 neutropenia in our study (72.4%; 7 days) was similar to what was observed in the MajesTEC-1 study (65.5%; 8 days).<span><sup>8</sup></span> However, the median time to onset of grade ≥3 neutropenia was shorter in our study compared to the MajesTEC-1 study (19 vs. 69 days).<span><sup>8</sup></span> The use of granulocyte-colony-stimulating factor support was comparable with or without prophylactic tocilizumab (62.1% vs. 54.5%).<span><sup>8</sup></span></p><p>Our data indicate that prophylaxis with tocilizumab prior to step-up dose 1 results in a marked reduction in the occurrence of teclistamab-induced CRS without a negative impact on response or PFS, despite a high proportion of patients with high-risk cytogenetic abnormalities or extramedullary disease. This is in line with other studies which also showed that tocilizumab does not compromise the therapeutic activity of CAR T cells or BsAbs targeting other MM-associated antigens.<span><sup>4, 9-11</sup></span></p><p>Two additional studies have evaluated prophylactic tocilizumab with the aim of reducing the CRS rate with teclistamab: another single-center study,<span><sup>12</sup></span> and the prophylactic tocilizumab cohort of the MajesTEC-1 study.<span><sup>13, 14</sup></span> In the single-center study, tocilizumab was administered prophylactically prior to the second step-up dose in 38 patients.<span><sup>12</sup></span> CRS occurred in 26.3% of these patients (grade 1: 21.1%; grade 2: 2.6%; grade ≥3: 2.6%).<span><sup>12</sup></span> Notably, half of the CRS events occurred after step-up dose 1, and these patients received tocilizumab treatment rather than prophylaxis.<span><sup>12</sup></span> Our study with a lower rate of CRS suggests that the optimal timing of prophylactic tocilizumab administration is prior to step-up dose 1. However, tocilizumab was also given ≤4 h prior to the first step-up dose in the prophylactic tocilizumab cohort of the MajesTEC-1 study (<i>n</i> = 24), with a higher CRS rate (25.0% [grade 1: 8.3%; grade 2: 16.7%; no grade ≥3 events]), compared to what was observed in our patients.<span><sup>13, 14</sup></span> The different CRS frequencies in these two studies evaluating tocilizumab prior to the first step-up dose are potentially related to heterogeneity in patient- and disease characteristics. It is unlikely that the slightly different timing of tocilizumab administration (1 vs. ≤4 h prior to the first step-up dose) explains the different CRS frequency given and the long half-life of tocilizumab.<span><sup>7</sup></span></p><p>It is expected that tocilizumab prophylaxis will prevent delays in dosing and prolongation of hospital stay with teclistamab. Preventing CRS is also important for patients with heart failure and severe renal impairment (especially those receiving hemodialysis) to avoid hypotension, which may necessitate the administration of IV fluids with a risk of subsequent fluid overload. CRS should also be prevented in rare conditions where fever provokes cardiac arrhythmias, such as in Brugada syndrome. In addition, prophylactic tocilizumab has the potential to reduce the use of steroids for CRS management, which is associated with a higher risk of infectious complications following initiation of BsAb treatment.<span><sup>15</sup></span> Our data also support the further evaluation of prophylactic tocilizumab to enable safe outpatient teclistamab administration, which has the potential to reduce healthcare resource utilization and improve patients' quality of life.</p><p>A limitation of our study is that outside clinical trials BM examination was not always performed to define CR. In addition, the sample size in this analysis was too small for definitive conclusions about disease- or patient-related factors that predict CRS despite tocilizumab prophylaxis. However, our results and those from another study<span><sup>12</sup></span> suggest that a high frequency of circulating plasma cells may be associated with grade ≥2 CRS, despite tocilizumab prophylaxis. New studies with larger numbers of patients are needed to evaluate which baseline characteristics are predictive of CRS in patients receiving tocilizumab prophylaxis. In addition, a subset of patients did not develop CRS in the pivotal cohort of MajesTEC-1,<span><sup>4</sup></span> indicating that with the prophylactic tocilizumab strategy, we also exposed patients to tocilizumab who would not have needed it. Unfortunately, at this moment, it is not possible to reliably identify patients who will develop CRS.<span><sup>4</sup></span></p><p>In conclusion, prophylactic tocilizumab administered prior to step-up dose 1 markedly reduced the frequency of CRS without affecting efficacy. Although step-up dosing is commonly administered in an inpatient setting, we also demonstrate that the low CRS rate with tocilizumab prophylaxis may improve the safety and feasibility of outpatient teclistamab step-up dosing with a low risk of admission to the hospital for CRS treatment.</p><p>Niels W. C. J. van de Donk designed the study. Charlotte L. B. M. Korst, Kaz Groen, Patricia W. C. Bosman, Fleur van der Valk, Christie P. M. Verkleij, Sandy Kruyswijk, Maaike E. M. de Ruijter, Dianne M. Heijink, Maria T. Kuipers, Sonja Zweegman, and Niels W. C. J. van de Donk enrolled patients, contributed data, and interpreted data. Charlotte L. B. M. Korst and Niels W. C. J. van de Donk designed and performed statistical analyses. Niels W. C. J. van de Donk drafted the first version of the manuscript, and all authors had access to all the data reported in the study and revised and approved the final version of the manuscript.</p><p>Sonja Zweegman has received research funding from Celgene, Takeda, and Janssen and serves on advisory boards for Janssen, Takeda, BMS, Oncopeptides, and Sanofi, all paid to the institution. Niels W. C. J. van de Donk has received research support from Janssen Pharmaceuticals, AMGEN, Celgene, Novartis, Cellectis, and BMS and serves on advisory boards for Janssen Pharmaceuticals, AMGEN, Celgene, BMS, Takeda, Merck, Roche, Novartis, Bayer, Adaptive, Pfizer, Abbvie, and Servier, all paid to the institution. The remaining authors declare no conflict of interest.</p><p>The teclistamab compassionate use program and MajesTEC-1 study were supported by Janssen Pharmaceuticals.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 7","pages":""},"PeriodicalIF":7.6000,"publicationDate":"2024-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11266829/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.132","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Teclistamab, a T-cell redirecting bispecific antibody (BsAb) targeting B-cell maturation antigen (BCMA), has marked activity in heavily pretreated multiple myeloma (MM) patients (overall response rate: 63.0%; at least very good partial response [≥VGPR]: 59.4%; median progression-free survival [PFS]: 11.3 months).1, 2 Teclistamab treatment induces T-cell activation and production of proinflammatory cytokines such as interleukin-6 (IL-6).3 This increase in cytokines frequently results in a systemic inflammatory response syndrome (cytokine-release syndrome [CRS]), characterized by fever, and in more severe cases also hypotension and hypoxia.1, 2, 4, 5 CRS mitigation strategies include step-up dosing and premedication with steroids and antihistamines. The incidence of CRS in teclistamab-treated patients was 72.1% (grade 2: 21.2%; grade ≥3: 0.6%) with most CRS events occurring during step-up dosing.1, 2, 4 Recurrent CRS occurred in 33.3% of the patients.4 Patients are generally hospitalized for the administration of the step-up doses and first full dose to adequately monitor for early signs and symptoms of CRS (median hospital stay in a real-world setting: 10 days).1, 6 Treatment of CRS with steroids or the IL-6 receptor-blocking antibody tocilizumab is effective with rapid resolution of symptoms.3, 4 Patients who received tocilizumab for their first CRS event were less likely to experience a subsequent CRS event compared to those who did not receive tocilizumab (20.0% vs. 62.2%).4 A single dose of tocilizumab blocks the IL-6 receptor for approximately 10 days and covers the full step-up dosing period.7 Based on these data, we aimed to evaluate the efficacy of tocilizumab administered prior to the first step-up dose to prevent the development of CRS following the initiation of teclistamab therapy in 29 patients treated in our hospital.
Teclistamab was administered according to the approved schedule with two step-up doses (0.06 and 0.3 mg/kg) followed by the full dose of 1.5 mg/kg every week (48–72 h between step-up doses and the first full dose). In patients undergoing hemodialysis, teclistamab was given directly after hemodialysis sessions. Prophylactic tocilizumab (8 mg/kg intravenously [IV]; maximum dose of 800 mg) was administered 1 h prior to the first step-up dose. Patients also received 16 mg dexamethasone, 2 mg clemastine, and 1000 mg acetaminophen 1 h prior to both step-up doses and the first full dose. All patients received herpes zoster (valacyclovir) and Pneumocystis jirovecii pneumonia prophylaxis (co-trimoxazole, or pentamidine in case of co-trimoxazole allergy). Granulocyte colony-stimulating factor was considered in cases of grade ≥3 neutropenia, and IgG replacement was given in cases with polyclonal IgG <4 g/L (either as primary or secondary prophylaxis at individual physician's discretion). At the current follow-up, 26 patients (89.7%) received IgG replacement. Patients did not receive other antibacterial or antifungal prophylaxis. CRS and immune effector cell-associated neurotoxicity syndrome (ICANS) were graded according to the American Society for Transplantation and Cellular Therapy criteria.5
Prophylactic tocilizumab was given from October 2022 to March 2024 to all relapsed/refractory MM patients who received teclistamab monotherapy as part of a compassionate use program (CUP; n = 20) and also to nine consecutive patients who received teclistamab in the MajesTEC-1 trial1 (total number of patients: 29). The study site ethics committee approved the protocols, which were conducted according to the principles of the Declaration of Helsinki, the International Conference on Harmonization, and the Guidelines for Good Clinical Practice. All patients provided written informed consent.
Patient characteristics are shown in Table 1. Patients had received a median of four prior lines of therapy. None of the patients had prior exposure to a BCMA-directed therapy, and only one patient was previously treated with a non-BCMA-targeting BsAb (talquetamab). The majority of the CUP patients (90%) would not have met the eligibility criteria for MajesTEC-1 due to the presence of oligosecretory disease (n = 7), severe cytopenias (n = 7), renal impairment (n = 3, including hemodialysis in one patient), cardiac conditions (n = 2, one patient with heart failure [New York Heart Association class III] and one with Brugada syndrome), and/or other reasons.
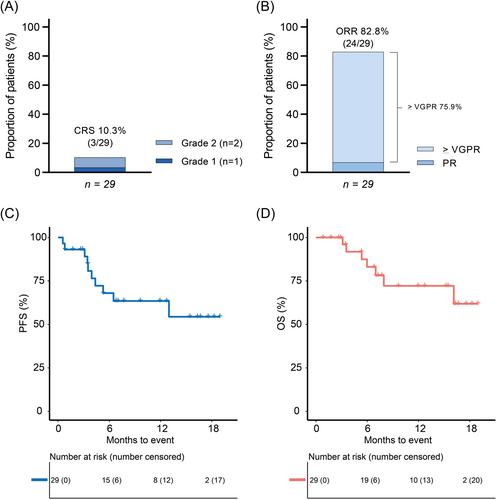
CRS occurred in only three of the 29 patients (10.3%); one patient with grade 1 CRS after step-up dose 1, one patient with grade 2 CRS after step-up dose 1, and one patient with grade 1 CRS after step-up dose 2 and grade 2 CRS after the first full dose (Figure 1A). CRS treatment consisted of additional tocilizumab administration in all three patients and dexamethasone (10 mg IV) in the patient with recurrent CRS. Both patients with grade 2 CRS also received IV fluids because of hypotension. The median duration of CRS was one day (range, 1–3). All CRS events were resolved completely.
Both patients who developed grade 2 CRS despite prophylactic tocilizumab had high tumor burden (70%–80% MM cells in bone marrow [BM] biopsy) and rapidly progressive disease (light-chain doubling time of approximately 4 weeks prior to initiation of teclistamab treatment), which was not the case in the patient with grade 1 CRS (30% MM cells in BM biopsy; increase in light-chain level by 25% during the 4 weeks prior to the first teclistamab dose). Evaluation of the peripheral blood smears by conventional microscopy revealed circulating tumor cells in one of the three patients who developed CRS (patient with recurrent CRS). Circulating tumor cells were not detected in the blood smear of patients who did not develop CRS.
Twenty-five patients received teclistamab step-up dosing in the inpatient setting. The median duration of hospitalization for step-up dosing was 8 days (interquartile range, 6–9 days), with only one patient staying 2 days longer than expected because of grade 2 CRS after the first full dose. Notably, four patients received teclistamab step-up dosing in the outpatient setting with tocilizumab prophylaxis without the development of CRS or the need for hospitalization. These patients lived relatively close to the hospital (<60 min travel time) and were in the company of a competent adult.
Overall, tocilizumab prophylaxis had no negative impact on the activity of teclistamab with 24 of the 29 patients (82.8%) achieving a partial response or better with ≥VGPR in 75.9%. With a median follow-up of 8.7 months, the median PFS was not reached (12-month PFS: 63.5%). OS at 12 months was 72.2% (Figure 1B–D). All three patients with renal impairment responded, including the patient who received hemodialysis (VGPR). Except for the lower CRS rate, the safety profile of teclistamab with prophylactic tocilizumab was comparable to that observed in the MajesTEC-1 trial1, 2 with grade ≥3 thrombocytopenia in 13.8%, grade ≥3 anemia in 6.9%, and grade ≥3 infections in 27.6%. ICANS, which typically concurs with CRS, was observed in none of the 29 patients. Also, the frequency and median duration of grade ≥3 neutropenia in our study (72.4%; 7 days) was similar to what was observed in the MajesTEC-1 study (65.5%; 8 days).8 However, the median time to onset of grade ≥3 neutropenia was shorter in our study compared to the MajesTEC-1 study (19 vs. 69 days).8 The use of granulocyte-colony-stimulating factor support was comparable with or without prophylactic tocilizumab (62.1% vs. 54.5%).8
Our data indicate that prophylaxis with tocilizumab prior to step-up dose 1 results in a marked reduction in the occurrence of teclistamab-induced CRS without a negative impact on response or PFS, despite a high proportion of patients with high-risk cytogenetic abnormalities or extramedullary disease. This is in line with other studies which also showed that tocilizumab does not compromise the therapeutic activity of CAR T cells or BsAbs targeting other MM-associated antigens.4, 9-11
Two additional studies have evaluated prophylactic tocilizumab with the aim of reducing the CRS rate with teclistamab: another single-center study,12 and the prophylactic tocilizumab cohort of the MajesTEC-1 study.13, 14 In the single-center study, tocilizumab was administered prophylactically prior to the second step-up dose in 38 patients.12 CRS occurred in 26.3% of these patients (grade 1: 21.1%; grade 2: 2.6%; grade ≥3: 2.6%).12 Notably, half of the CRS events occurred after step-up dose 1, and these patients received tocilizumab treatment rather than prophylaxis.12 Our study with a lower rate of CRS suggests that the optimal timing of prophylactic tocilizumab administration is prior to step-up dose 1. However, tocilizumab was also given ≤4 h prior to the first step-up dose in the prophylactic tocilizumab cohort of the MajesTEC-1 study (n = 24), with a higher CRS rate (25.0% [grade 1: 8.3%; grade 2: 16.7%; no grade ≥3 events]), compared to what was observed in our patients.13, 14 The different CRS frequencies in these two studies evaluating tocilizumab prior to the first step-up dose are potentially related to heterogeneity in patient- and disease characteristics. It is unlikely that the slightly different timing of tocilizumab administration (1 vs. ≤4 h prior to the first step-up dose) explains the different CRS frequency given and the long half-life of tocilizumab.7
It is expected that tocilizumab prophylaxis will prevent delays in dosing and prolongation of hospital stay with teclistamab. Preventing CRS is also important for patients with heart failure and severe renal impairment (especially those receiving hemodialysis) to avoid hypotension, which may necessitate the administration of IV fluids with a risk of subsequent fluid overload. CRS should also be prevented in rare conditions where fever provokes cardiac arrhythmias, such as in Brugada syndrome. In addition, prophylactic tocilizumab has the potential to reduce the use of steroids for CRS management, which is associated with a higher risk of infectious complications following initiation of BsAb treatment.15 Our data also support the further evaluation of prophylactic tocilizumab to enable safe outpatient teclistamab administration, which has the potential to reduce healthcare resource utilization and improve patients' quality of life.
A limitation of our study is that outside clinical trials BM examination was not always performed to define CR. In addition, the sample size in this analysis was too small for definitive conclusions about disease- or patient-related factors that predict CRS despite tocilizumab prophylaxis. However, our results and those from another study12 suggest that a high frequency of circulating plasma cells may be associated with grade ≥2 CRS, despite tocilizumab prophylaxis. New studies with larger numbers of patients are needed to evaluate which baseline characteristics are predictive of CRS in patients receiving tocilizumab prophylaxis. In addition, a subset of patients did not develop CRS in the pivotal cohort of MajesTEC-1,4 indicating that with the prophylactic tocilizumab strategy, we also exposed patients to tocilizumab who would not have needed it. Unfortunately, at this moment, it is not possible to reliably identify patients who will develop CRS.4
In conclusion, prophylactic tocilizumab administered prior to step-up dose 1 markedly reduced the frequency of CRS without affecting efficacy. Although step-up dosing is commonly administered in an inpatient setting, we also demonstrate that the low CRS rate with tocilizumab prophylaxis may improve the safety and feasibility of outpatient teclistamab step-up dosing with a low risk of admission to the hospital for CRS treatment.
Niels W. C. J. van de Donk designed the study. Charlotte L. B. M. Korst, Kaz Groen, Patricia W. C. Bosman, Fleur van der Valk, Christie P. M. Verkleij, Sandy Kruyswijk, Maaike E. M. de Ruijter, Dianne M. Heijink, Maria T. Kuipers, Sonja Zweegman, and Niels W. C. J. van de Donk enrolled patients, contributed data, and interpreted data. Charlotte L. B. M. Korst and Niels W. C. J. van de Donk designed and performed statistical analyses. Niels W. C. J. van de Donk drafted the first version of the manuscript, and all authors had access to all the data reported in the study and revised and approved the final version of the manuscript.
Sonja Zweegman has received research funding from Celgene, Takeda, and Janssen and serves on advisory boards for Janssen, Takeda, BMS, Oncopeptides, and Sanofi, all paid to the institution. Niels W. C. J. van de Donk has received research support from Janssen Pharmaceuticals, AMGEN, Celgene, Novartis, Cellectis, and BMS and serves on advisory boards for Janssen Pharmaceuticals, AMGEN, Celgene, BMS, Takeda, Merck, Roche, Novartis, Bayer, Adaptive, Pfizer, Abbvie, and Servier, all paid to the institution. The remaining authors declare no conflict of interest.
The teclistamab compassionate use program and MajesTEC-1 study were supported by Janssen Pharmaceuticals.
此外,预防性托珠单抗有可能减少类固醇在CRS治疗中的使用,而类固醇与开始BsAb治疗后较高的感染性并发症风险有关15。我们的数据还支持进一步评估预防性托珠单抗,以实现门诊患者安全使用替卡单抗,这有可能减少医疗资源的使用并改善患者的生活质量。此外,这项分析的样本量太小,无法就预测托珠单抗预防后 CRS 的疾病或患者相关因素得出明确结论。然而,我们的结果和另一项研究12 的结果表明,尽管使用了托珠单抗预防治疗,但循环浆细胞的高频率可能与≥2 级 CRS 相关。需要对更多患者进行新的研究,以评估哪些基线特征可预测接受托西珠单抗预防治疗的患者的 CRS。此外,在 MajesTEC-1 的关键队列中,有一部分患者没有发生 CRS,4 这表明,在预防性使用托珠单抗的策略中,我们也让原本不需要使用托珠单抗的患者接触到了托珠单抗。遗憾的是,目前还无法可靠地确定哪些患者会发生 CRS。4 总之,在加大剂量 1 之前使用预防性托珠单抗明显降低了 CRS 的发生频率,而且不影响疗效。虽然递增剂量通常在住院环境中进行,但我们也证明了预防性使用托西珠单抗的低CRS率可能会提高门诊特克司他单抗递增剂量的安全性和可行性,同时降低入院治疗CRS的风险。Charlotte L. B. M. Korst、Kaz Groen、Patricia W. C. Bosman、Fleur van der Valk、Christie P. M. Verkleij、Sandy Kruyswijk、Maaike E. M. de Ruijter、Dianne M. Heijink、Maria T. Kuipers、Sonja Zweegman和Niels W. C. J. van de Donk招募患者、提供数据并解释数据。Charlotte L. B. M. Korst 和 Niels W. C. J. van de Donk 设计并进行了统计分析。Niels W. C. J. van de Donk 起草了手稿的第一版,所有作者均可获得研究中报告的所有数据,并修改和批准了手稿的最终版本。Sonja Zweegman 曾获得 Celgene、武田和杨森的研究资助,并在杨森、武田、BMS、Oncopeptides 和赛诺菲的顾问委员会任职,所有报酬均由该机构支付。Niels W. C. J. van de Donk 获得了杨森制药、AMGEN、Celgene、诺华、Cellectis 和 BMS 的研究资助,并在杨森制药、AMGEN、Celgene、BMS、武田、默克、罗氏、诺华、拜耳、Adaptive、辉瑞、艾伯维和赛维耶的顾问委员会任职,所有这些机构均向其支付报酬。其余作者声明没有利益冲突。泰克司他单抗同情使用计划和MajesTEC-1研究得到了杨森制药公司的支持。
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


