Speech–language therapy services for children with cleft palate: A scoping review on continuity of care
Abstract
Background
Children with a cleft palate (with or without a cleft of the lip) often require speech–language therapy (SLT) services to achieve age-appropriate speech. For many children, this involves attending SLT services delivered by both specialised cleft team speech–language therapists (SLTs) and a local, community or school-based SLT. Given that these two different SLTs are typically involved in the child's care, it is important to ensure that effective communication, coordination and collaboration occur between them. This is known as continuity of care. While continuity of care in speech therapy has not generally been evaluated, in medicine it has been shown to improve health outcomes.
Aims
To identify what is known from the existing literature about processes for continuity of care in cleft speech therapy services.
Methods & Procedures
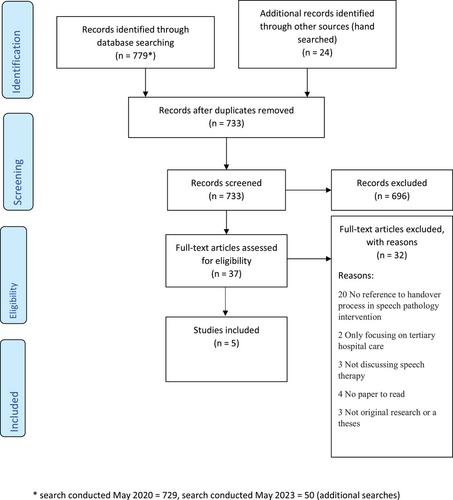
A scoping review was conducted using Arksey and O'Malley's methodological framework. Seven databases were searched including MEDLINE via OVID, EMBASE via OVID, CINAHL via EBSCO, PsychINFO, Scopus, Web of Science and SpeechBITE. Covidence was used to screen 733 initial articles and five studies met the inclusion criteria. Thematic analysis was conducted to identify global and subthemes.
Main Contribution
Five papers were included for analysis. These identified two salient characteristics of cleft speech therapy continuity of care: (1) it is a continuous cycle and (2) it is complex. Although parents are integral team members, cleft and community SLTs must be responsible for initiating communication and collaborating. Furthermore, cleft SLTs have a crucial role in disseminating information and resources, as well as offering guidance and support.
Conclusions & Implications
Given that only five studies were included, there is a need to gather more information from parents, community SLTs, and cleft SLTs to understand their experiences and perspectives. From what is known, there are breakdowns in the processes needed for continuity of care, including confusion regarding roles and responsibilities, and community SLTs lacking confidence, knowledge and support. Recommendations are provided to facilitate improvements in continuity of care.
WHAT THIS PAPER ADDS
What is already known on the subject
-
Children with CP±L often require SLT from two different clinicians including a specialised cleft SLT and a community or school-based SLT. As such, it is important that effective communication and collaboration occur between them to ensure continuity of care.
What this study adds to the existing knowledge
-
This study identified a breakdown in the processes necessary for continuity of care. According to community SLTs, there is a discrepancy between their expectations and current practices. This scoping review has identified two critical characteristics of effective continuity of care: (1) it operates as an ongoing cycle; and (2) it is a complex, multifaceted endeavour.
What are the practical and clinical implications of this work?
-
This study highlights the importance of cleft and community SLTs taking the initiative in communication and collaboration, rather than solely relying on parents as intermediaries. By offering practical recommendations, this research aims to improve continuity of care, potentially fostering greater awareness and advancements in service delivery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


